

Things are not always what they seem; the first appearance deceives many; the intelligence of a few perceives what has been carefully hidden. — Roman poet Phaedrus
The simplest classification of foot type is to distinguish between a flat foot and one with a high arch. Pes planus, common in the general population, is characterized by a low or flat arch. It may be free of symptoms or associated with foot pain and altered biomechanics of the lower limb. Pes cavus describes a high arched foot that is less flexible. The typical presentation also includes an inverted, varus hindfoot and an adducted forefoot. Separating by type across these basic divisions is helpful, especially when first learning about the foot. It provides a basis for beginners to externally observe and group feet based on arch height, forefoot position, and calcaneal angle.
The Flattening Foot
What about the foot that has a high arch when the patient is seated in the exam chair and then becomes low arched when they stand? Which foot type do they have—and where did the arch go? An actual low arched foot will appear flat when the patient is seated and when he or she is standing. Likewise, a true pes cavus foot maintains its architecture when loaded and compensates accordingly. Longitudinal arch collapse, non-weight bearing to weight bearing, can occur for many reasons including ligamentous laxity, over-loading, impaired structural development, systemic disease, equinus, leg length discrepancy, and trauma. However, accepting these possible etiologies, it is still important to recognize the essential underlying foot structure.
Anterior Cavus
Pes cavus itself can be subdivided into categories of hindfoot, forefoot, or global (i.e., both). The classic rearfoot or posterior cavus has a severe varus alignment and a high calcaneal pitch, or angle, exceeding 30 degrees. Forefoot or anterior cavus is recognized by plantarflexion of the forefoot on the rearfoot: a downward angulation occurring in the midfoot. This foot type will have an arch when non-weight bearing but, depending on its compensation mechanism, it may disappear when standing.
Anterior cavus, also known as anterior equinus, can occur at several locations in the foot. With metatarsus cavus, the sagittal plane declination
is at Lisfranc’s joint (Figure 1) and is frequently seen as a plantarflexed first metatarsal. Moving proximally, lesser tarsus cavus occurs at the junction of the navicular and cuneiforms (Figure 2). Lastly, forefoot cavus is noted at Chopart’s joint (Figure 3). These types may also occur in combination. In each case there is a tell-tale characteristic localized bony prominence on the dorsum of the foot, and the heel naturally resides above the inclined forefoot—at least until it is weight bearing. Aspects of this foot type have also been referred to as functional forefoot drop (FFD). *1

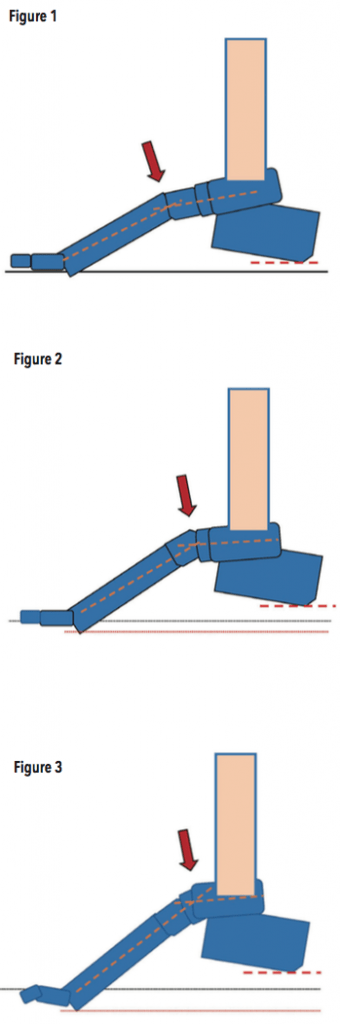
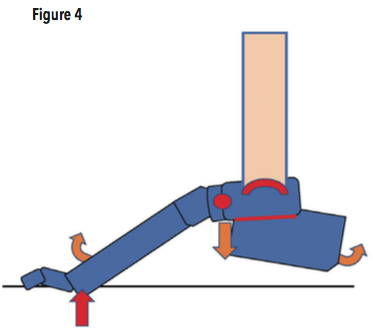
Ideal normal gait requires 10 degrees of dorsiflexion of the tibia over the plantigrade foot. If this is not available, there is an ankle equinus present and a series of foot pathologies can arise (see “Equinus” The O&P Edge, April 2013). In the foot with anterior cavus, due to the inherent plantarflexion of the forefoot, the ground reaction forces acting on the metatarsals push and dorsiflex them upward. The heel will come down to the ground, but it forces compensatory adaptation either at the midtarsal joint, the ankle, or the rearfoot (Figure 4). In doing so, the arch may collapse and appear flat, but this is not a pes planus. The term pseudoequinus was developed to describe this condition in which the forefoot equinus attitude uses up limited available talocrural joint motion. *2

Examination
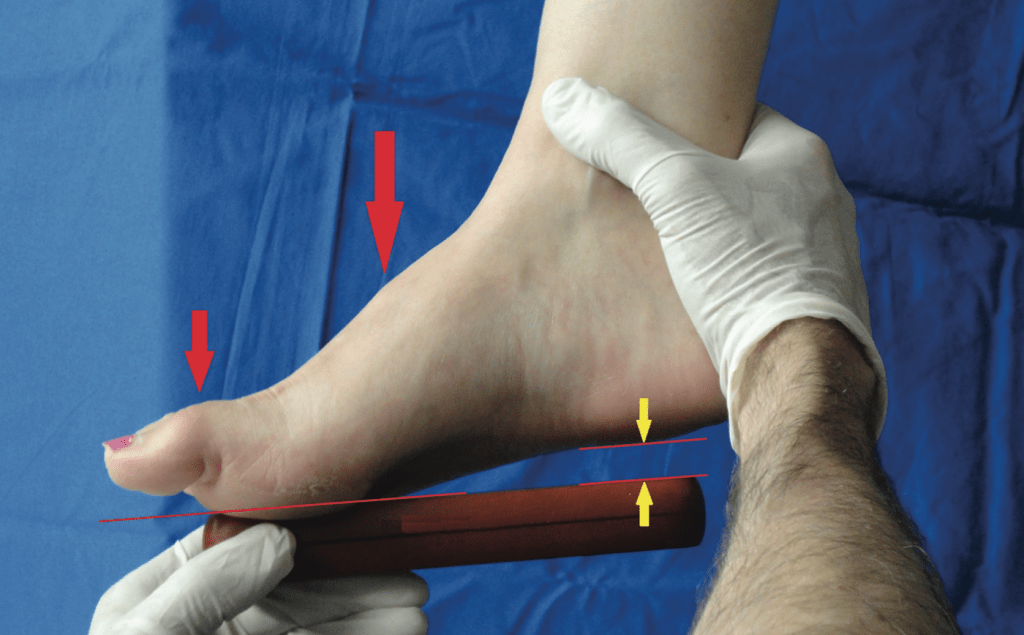
To recognize this foot type, first observe the non-weight bearing foot. With the rearfoot in the neutral position see if there is an arch present and if the forefoot angles downward (Figure 5).

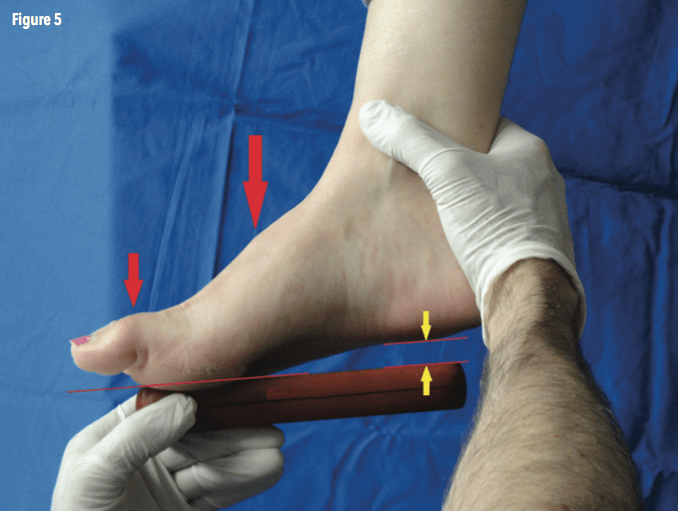
Look for a general prominence on the dorsum of the foot and note if the inclination is only on the medial or lateral column. It is not unusual to find retracted digits or hammer toes. Patients with anterior cavus often report discomfort wearing flat-soled shoes or flip-flops and do better in footwear with heels. They may also have previously rejected rigid orthotics that were designed to treat a flat foot as this foot type does not really need arch support, it needs a lift to fill the gap under the heel. If you suspect an anterior cavus, have the patient stand barefoot on bilateral heel lifts and see if the arch height is restored. Accommodative molds made from EVA or cork, or a semi-flexible device with a low durometer arch fill usually work well. Incorporate an appropriate heel elevation that allows the forefoot to rest in its natural plantarflexion. If there is a plantarflexed first ray, the design should also include a reversed Morton’s extension.
Conclusion
There is a lot more to foot function and pathology than outward appearance and shape. The pes planus foot may be quite stable, and a low arched foot with only mild pronation can be free of symptoms. Conversely, rigid cavus feet retain an arch when the person is either seated or standing. Certain anterior cavus feet have an arch that disappears upon weight bearing, but they should not be confused with traditional flatfoot. Anterior cavus is one type of a group sometimes referred to as “collapsible cavus” feet and can be treated using lifts, orthotics, and shoe gear with suitable heel elevations. *3 The O&PEDGE
Séamus Kennedy, BEng (Mech), CPed, is president and co-owner of Hersco Ortho Labs, New York. He can be contacted via e-mail at seamus@hersco.com or by visiting www.hersco.com.
The author gratefully acknowledges the help and contribution of Joseph C. D’Amico DPM, DSc in preparing this article.
*References
- Glancy, J. 2000. Control of the Foot /Ankle Complex: Orthotic Recommendations.
- Whitney, A. K., Green D. R. 1982. Pseudoequinus.
Journal of the American Podiatric Medical Association
72(7):365-71. PMID:7108111 - D’Amico, J. C. 2017. Emerging Insights On The Collapsible Cavus. Podiatry Today 30(2):42-51.