Running has been referred to as the king of all workouts. It is an activity that has been embraced at varying levels of competence by nearly 11 million adults in the United States alone, according to the American Running Association. Running doesn’t require the purchase or use of expensive equipment; it is possible to do it indoors or outdoors, usually year round. Not only does running provide a fantastic cardiovascular workout, it allows you to burn calories and clear your mind, leaving you with that relaxed, feel-good sense for many hours afterward. However, to reap these benefits on an ongoing basis, it is important to take precautions to prevent debilitating injuries.
For all the benefits of this great activity, there is no doubt that the repetitive nature of the stress it places on key joints can lead to breakdown. While there is some debate about what constitutes an injury, it has been estimated that up to 70 percent of runners will sustain some form of overuse injury during any one-year period. Anyone working in the orthotics, biomechanics, or sports medicine professions will see his or her fair share of running injuries. These injuries can be broadly classified as acute or chronic. Acute injuries are those due to sudden motions or twisting, such as an ankle sprain, which lead to soft tissue and/or osseous injury. These need to be treated immediately and allowed to heal.
Chronic injuries develop over time and are the result of repetitive stress that eventually leads to breakdown; e.g., patellofemoral syndrome. Chronic injuries account for well over 80 percent of running injuries, and they can develop from either an anatomical cause or a biomechanical issue and sometimes a combination of both. Because of its impact forces on the body, running greatly magnifies the extent of these anomalies. When experienced runners develop a chronic injury, it is often necessary to investigate what they have changed in their training practices.
To get a clear picture of any injury, it is necessary to do a full biomechanical exam. Evaluate the patient in stance and motion, non-weight bearing and weight bearing, in shoes and out of shoes. It is vital to follow the entire kinetic chain, not just treat the symptom, to investigate the root cause of the problem. John Connors, DPM, a New York-based sports-medicine specialist, insists on watching his patients function in order to determine underlying causes. He will even run with his world-class patients in order to diagnose their etiology.
Common Running Injuries
Heel pain: Heel pain is a common complaint among runners. This is hardly surprising, given that the majority of runners who train on level ground at low to moderate speeds are heel strikers. This running style produces an impact-force peak early in the stance phase, which can range from one-and-a-half to five times the runner’s body weight. These impact forces are considered a primary cause of overuse injuries.
The classic sign of plantar fasciitis (PF) is heel pain that presents first thing in the morning and then decreases with activity. In the early stages, the patient usually can still exercise, only to be faced with more severe pain following a run. Typically, pain will be felt at the plantar-medial aspect of the calcaneus or at the middle aspect of the calcaneus.
There are other causes of heel pain that should not be ruled out without further radiographic examination. A calcaneal stress fracture may present like PF, but typically the pain does not subside as the day progresses. A positive calcaneal compression test can indicate the presence of such a fracture. Other considerations for heel pain include tarsal tunnel syndrome, neuritis of the first branch of the lateral plantar nerve, and tendinitis of the flexor hallucis longus.
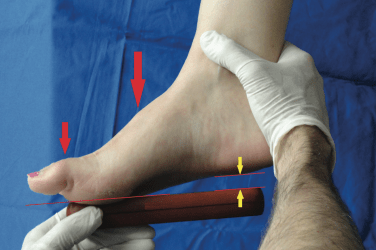
Achilles tendinitis (AT): Achilles tendon injuries may be due to inflammation of the paratenon or the result of the degeneration of the tendon itself. It is broadly classified into two groups: insertional (occurring at the tendon/bone interface) and non-insertional (occurring proximal to its insertion, in or about the tendon proper). A physician’s diagnosis will confirm the location and type of condition. AT can develop when the tendon contracts and tightens and is then over-stretched during exercise. There may also be a biomechanical component to the condition, given the tendon’s broad insertion on the posterior calcaneus. Due to the cyclic rotation of the STJ from pronation through supination, there can be increased tension on the medial and lateral aspects of the tendon’s insertion.
Iliotibial band syndrome (ITBS): This is a debilitating injury that presents as pain along the lateral aspect of the knee joint. It is sometimes accompanied by a clicking sensation. Current thinking is that ITBS results from weak core and hip muscles that fail to prevent tightening and strain the IT band.
Medial tibial stress syndrome (MTSS): Commonly known as “shin splints,” this pain is typically noted along the lower third of the posterior medial surface of the tibia. It can often result from improper biomechanics or by not following the training considerations described earlier.
There are many other injuries that you are likely to see in runners such as posterior tibial tendon pain, knee pain, and a variety of stress fractures. Forefoot pathologies can include functional hallux limitus, sesamoiditis, and second metatarsal phalangeal joint (MPJ) capsulitis, in addition to regular blisters, corns, and neuromas. Much has been written on each of these conditions and their specific rehabilitation treatments. “How to Detect and Treat Running Injuries,” by Brian Fullem, DPM, (Podiatry Today, May 2005) covers the basics. It is an excellent resource.
 Preventative Measures
Preventative Measures
Over the years, I have developed a great love for running, so I can say from personal experience as well as patient interaction that nearly all running injuries result from training errors. I try to follow my own advice on injury prevention as outlined above. I begin a run by forcing myself to stretch; I change out my running shoes as necessary, even if they look almost new; and I vary my workouts with swimming, yoga, and sometimes bicycling to ensure adequate rest. I am pleased to say that I am injury free. However, when injuries do occur, treatment will generally follow a protocol of relieving pain, resting, icing, stretching, focused strengthening, and improving biomechanics. Good support from shoes and orthotics, good running form, and good training habits, such as always stretching, will prevent the return of many of these injuries. I believe foot orthotics, whether custom or not, play an essential role in keeping a runner injury free by aligning the body properly. Regardless of foot type, appropriate orthotics will increase shock absorption and prevent end-of-range-of motion, thus protecting tendons, muscles, and joints.
Another strategy for preventing running injuries is to advise your patients to modify their running style. Recently, I have begun using a technique called ChiRunning©. In essence, ChiRunning aims to lessen the forces that most runners experience by introducing a slight forward lean and a biomechanically efficient flow to their running style. It advocates running with relaxed lower legs and using a mid-foot strike to avoid the braking and impact of heel strike. Since adopting the ChiRunning approach, I have found running even more enjoyable, not to mention less strenuous.
Hopefully, armed with this information and more, you can help your runners achieve their goals.
Séamus Kennedy, BEng (Mech), CPed, is president and co-owner of Hersco Ortho Labs, New York, New York. He can be contacted via e-mail at seamus@hersco.com, or visitwww.hersco.com