Diabetes Mellitus is a disease where the body either does not produce enough insulin or becomes insulin resistant, and there are elevated levels of glucose in the blood stream. With time, high blood sugar has manifold effects including neuropathy due to the deterioration of the peripheral nerves. One of the results is loss of protective sensation. This occurs first where the nerves are finest, in the extremities, leaving them vulnerable to injury and ulceration. Patients with advanced neuropathy often complain of numbness, tingling or burning in their fingers, hands, toes or feet.
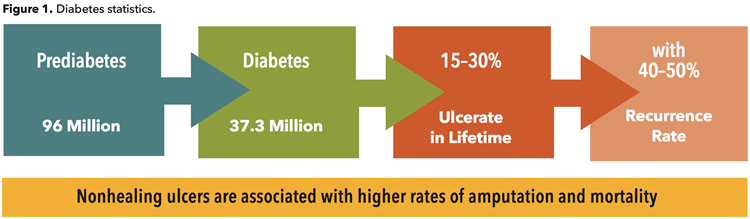
In addition, due to other complications from the disease, when skin breakdown occurs it is slow to heal, taking months or even years. This in turn can begin an expensive cycle of wound infections that may lead to amputation. Diabetes continues to be the number one cause of the approximately 150,000 amputations performed each year in the United States. According to the CDC, annually there are 154,000 hospitalizations associated with diabetic lower extremity amputations 1, which puts a huge financial burden on the healthcare system (Fig. 1).
Breakdown
Diabetic ulcers occur as a result of several factors including vascular issues, neuropathy and trauma to the skin. Typically, they manifest on the feet first as full body weight is repetitively transferred with every step. The possibility of a foot ulcer developing is in proportion to the extent of the neuropathy and the magnitude of shear force which can be conceptually represented as follows:
Neuropathy + Shear Force + Time = Ulcer
This simple formula also indicates how a diabetic patient can be protected. If the advancement of neuropathy can be halted, shear forces held below the threshold of breakdown or the number of damaging cycles limited, ulceration will not occur. However, none of these factors are static, each is liable to change.
Neuropathy
Clearly Neuropathy is the critical component, and limiting it represents the greatest opportunity to avoid the catastrophic cycle of pedal destruction. The goal is to keep patients up, moving and active so the single best approach is to focus on the root cause: Prevent neuropathy by educating patients, increasing awareness of the dangers, and promoting a healthy lifestyle.
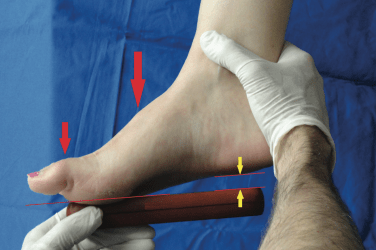
In response to the critical need for the prevention of foot ulcers the International Working Group on the Diabetic Foot has created an extensive archive of material for healthcare practitioners 2. This includes the initial exam, follow up and treatment plan based on the staging. Their foot screening protocol is an excellent guide to quickly evaluate and determine a patient’s risk category. They recommend all diabetic patients at risk for peripheral neuropathy be tested at a minimum annually using Semmes-Weinstein mono-filaments to record touch pressure sensation.
Shear Force
Although pressure is often cited as a causative factor of breakdown it is more correct to name shear force as the culprit. Pressure can be considered a proxy for shear, but they are different. Pressure is a measure of force applied over an area, and skin can withstand reasonable amounts of static pressure. However, shear is the active force when two adjacent surfaces move over each other. Whereas pressure acts down on a surface, shear is a result of sliding. It is possible to have pressure without shear, but you will not have shear without pressure. Poorly fitted footwear, either too tight or too loose, an incorrect shoe shape, or a low toe box can cause unnecessary rubbing and friction leading to blisters and eventually ulceration.
Shear force can be dramatically reduced by selecting proper shoes, sized correctly for the larger foot. Footwear for diabetics should have minimal seams, a smooth low friction lining, wide and high toe box and removable extra depth inlay. An ideal shoe supports the foot’s natural shape, has a slightly elevated heel (10 – 12mm drop), a closure that accommodates mild edema and full length total contact insoles. When neuropathy is more advanced patients benefit from customized insoles or custom orthotics fabricated to redistribute load and protect specific areas of high pressure. In the worst cases custom molded shoes may be prescribed.
As friction is a key component in the development of shear, patient skin condition is also crucial. Patients with diabetes often have dry, brittle skin. This is a consequence of poor circulation and glycosylation, an irreversible cross-linking of collagen and keratin which causes a thickening of the skin, tendons, ligaments, and joint capsules. The integrity of dry skin can be maintained using a prescribed moisturizer. Finally, hosiery is an important consideration. White socks that are thin on top with plantar padding, a loose non-constricting fit and seamless construction, especially at the toes, are less likely to precipitate a problem. It is also recommended to wear socks that are moisture wicking and breathable to prevent the buildup of bacteria.
Time
The component of time refers to both how long the patient has had neuropathy and how frequently shear force is experienced. Nerve damage, which is cumulative and non-reversible, occurs when blood sugars are out of control, beyond their recommended limit. The first line of defense is maintaining proper glucose and A1C levels.
Mechanical damage occurs when forces are above the threshold for destruction. Reducing the number of repetitions or lessening the friction causing shear limits this potential. Although not ideal there are ways to curtail the amount of time a patient spends walking. Part of the efficacy of Total Contact Casts and CROWs, if the patient will wear them, is that they impede mobility. Less steps equal less cyclical loading. Of course, these devices work in other important ways protecting the foot and reducing movement within the device.
Protecting the Forefoot
Due to a number of reasons the majority of diabetic foot ulcers occur in the forefoot. Firstly, this is where distal neuropathy begins to attack. Secondly, in terminal stance, the smaller area of the forefoot alone supports full body weight as the limb prepares for propulsion. Finally, in 3rd rocker, restrictions in joint range of motion can increase ground reaction force (GRF) distally (Fig 2).
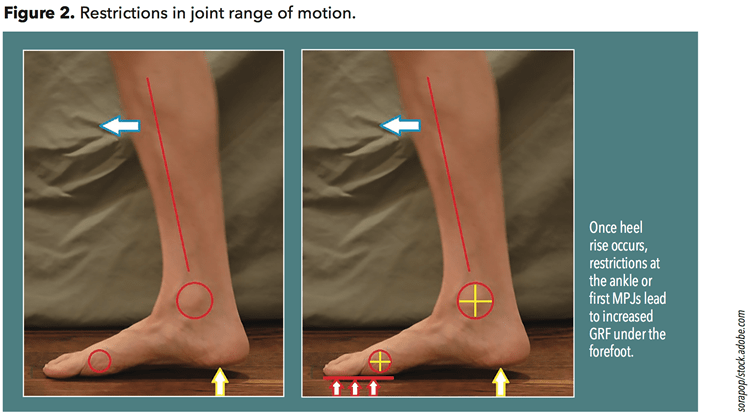
The smooth operation of the 1st MPJ is of immense importance 4. During terminal stance, once heel lift begins, the 1st MPJ is the pivot around which the body rotates. Functional Hallux Limitus is a restriction that occurs only when the joint is loaded. There is a distinct lack of motion at the 1st metatarsal head and a perceived locking of the joint. This can lead to a variety of compensations as the body naturally seeks alternate paths to continue forward. One possibility is to externally rotate and abduct the foot so that body weight passes over the side of the foot rather than through its long axis. These patients often have a pinch callus on the medial side of the hallux, a precursor for an ulcer. Inspection of the insole can reveal an absence of wear under the 1st met head, and clear indications of pressure under the great toe and sometimes the lesser mets.
Certain orthotic designs help restore some of this lost motion as plantarflexion of the 1st metatarsal bone aids hallux dorsiflexion. A well-fitting custom foot orthotic will raise the medial longitudinal arch, support the midfoot and maintain the 1st metatarsal in proper sloped alignment. In addition, accommodations can be made to allow the 1st met head to sit lower. A 1st ray cut-out in the orthotic shell slightly drops the 1st met head. Likewise, a reverse Morton’s extension provides a channel that the 1st met can sit into. A Kinetic Wedge is a rectangular cut-out distal to the orthotic shell that creates a depression for the 1st met head. These approaches allow the 1st met head to drop down, improve motion at the joint and they also serve to transfer some of the forces laterally.
Equinus is a common foot and ankle condition which is believed to be a leading contributor to foot pathology 5. In the case of diabetics with advanced neuropathy, it is strongly linked to the breakdown and ulceration of the forefoot. In simple terms equinus is the inability of the ankle joint to dorsiflex sufficiently which inhibits the body’s mass from passing over the plantigrade foot in 2nd rocker. Although there is no universal standard as to what constitutes equinus, a widely accepted value for static measurement of dorsiflexion at the ankle joint is 10 degrees. Any restriction in motion at the ankle joint, initiating early heel rise, means the insensate forefoot will be bearing body weight for longer, prolonging the time that the smaller area of the forefoot must sustain GRF.
The worst effects of equinus can be limited through the use of heel lifts that reduce the magnitude and duration of GRF acting under the forefoot. Conversely, full length solid ankle AFOs and CROWs, that restrict flexion at the ankle and met heads, also reduce peak pressure under the forefoot by maintaining the foot in midstance. Although they alter gait they may be a necessary compromise to protect the foot.
Rocker Soles
Rocker soles assist movement in the sagittal plane and lessen pressure under the forefoot. They are an aid to restoring fluid motion and the natural rockers of gait when there is a restriction, whether due to joint limitation or an orthotic device. Benefits include a reduction in GRF and compensation for rigid joints. It is possible to guide motion and disperse pressure by adjusting the angle of the fulcrum, its location and the pitch of sole.
In one study the biomechanical effects of prefab foot orthoses and rocker‐sole footwear was examined in individuals with 1st MPJ osteoarthritis (OA) 6. The subjects (n= 102) were randomly assigned either the orthotic or a rocker sole shoe and then wore both sensor motion analysis and in-shoe plantar pressure measurement systems. It was noted “the rocker-sole footwear resulted in reduced cadence, percentage of the gait cycle spent in stance phase, and sagittal plane hip range of motion”. Both interventions significantly reduced peak pressure under the first MTP joint, and the rocker-sole shoes also reduced peak pressure under the 2nd through 5th MTP joints and heel. They concluded in part “prefabricated foot orthoses and rocker-sole footwear are effective at reducing peak pressure under the 1st MTP joint…”. Although this study focused on patients with 1st MPJ OA it demonstrates the effectiveness of rocker soles in redistributing forefoot plantar pressures.
Conclusion
Patients with prediabetes have a blood glucose level that is above normal but not yet high enough to be classified diabetic. This stage is reversible. It remains the single best opportunity to curb the progress of this morbid epidemic. Educating patients and keeping them up and active remains the best medicine. Direct benefits include higher patient quality of life, and significantly lower health care costs. If neuropathy can be avoided in the first place the body will act as its own sentry against shear force and skin breakdown.
Once neuropathy takes hold vigilance is required to prevent injury by wearing proper fitting protective shoes and socks, and reducing pressure from weight bearing activities and ambulation. The feet must be inspected daily for signs of skin irritation, pre-ulcerative callusing or deformity. As the disease advances the patient’s biomechanics must be evaluated. It plays an important causative role in generating shear force and, if left unaddressed, healed ulcers are likely to reopen. Orthotic and pedorthic devices can be designed to limit the most destructive effects of shear force.
Séamus Kennedy, BEng (Mech), CPed, FAAOP(A) is president and co-owner of Hersco Ortho Labs, New York. He can be contacted via e-mail at seamus@hersco.com or by visiting www.hersco.com.
REFERENCES
- https://www.cdc.gov/diabetes/php/data-research/methods.html
- https://iwgdfguidelines.org/guidelines-2023/all-guidelines-2023/
- Physical Signs of the Intrinsic Minus Foot
Richard K. Bernstein
Diabetes Care 2003;26(6):1945–1946 PubMed:12766145 - Hallux Limitus and the Vital Operation of the First MPJ
The O&P Edge, May 2014 - Equinus
The O&P Edge, April 2013 - Biomechanical Effects of Prefabricated Foot Orthoses and Rocker‐Sole Footwear in Individuals With 1st Metatarsophalangeal Joint Osteoarthritis
Hylton B. Menz et al.
Arthritis Care Res 2016 May; 68(5): 603–611.