

An aponeurosis by definition is a broad flat sheet of dense fibrous connective tissue. The plantar fascia is an aponeurosis that serves as both a static and dynamic support structure of the foot. It is a broad ligamentous layer with its origin at the medial calcaneus and extends distally to the ball of the foot. There are also medial and lateral slips, but the central band provides the main support. This central band fans out across the midfoot and divides into a series of tracts with multiple insertions across the ligaments and fascia of all the metatarsal joints. Although the insertion of the Achilles tendon at the posterior calcaneus is distinct and separate from the origin of the plantar fascia, they are mechanically linked. Forces acting on the Achilles tendon transfer strain to the plantar fascia.

Inflammation or degeneration of the plantar fascia can occur at the insertion or along its course causing significant pain. Much research has been conducted to examine the strength and the function of the plantar aponeurosis in an attempt to understand conditions that may lead to pathology.
Trusses and Ties
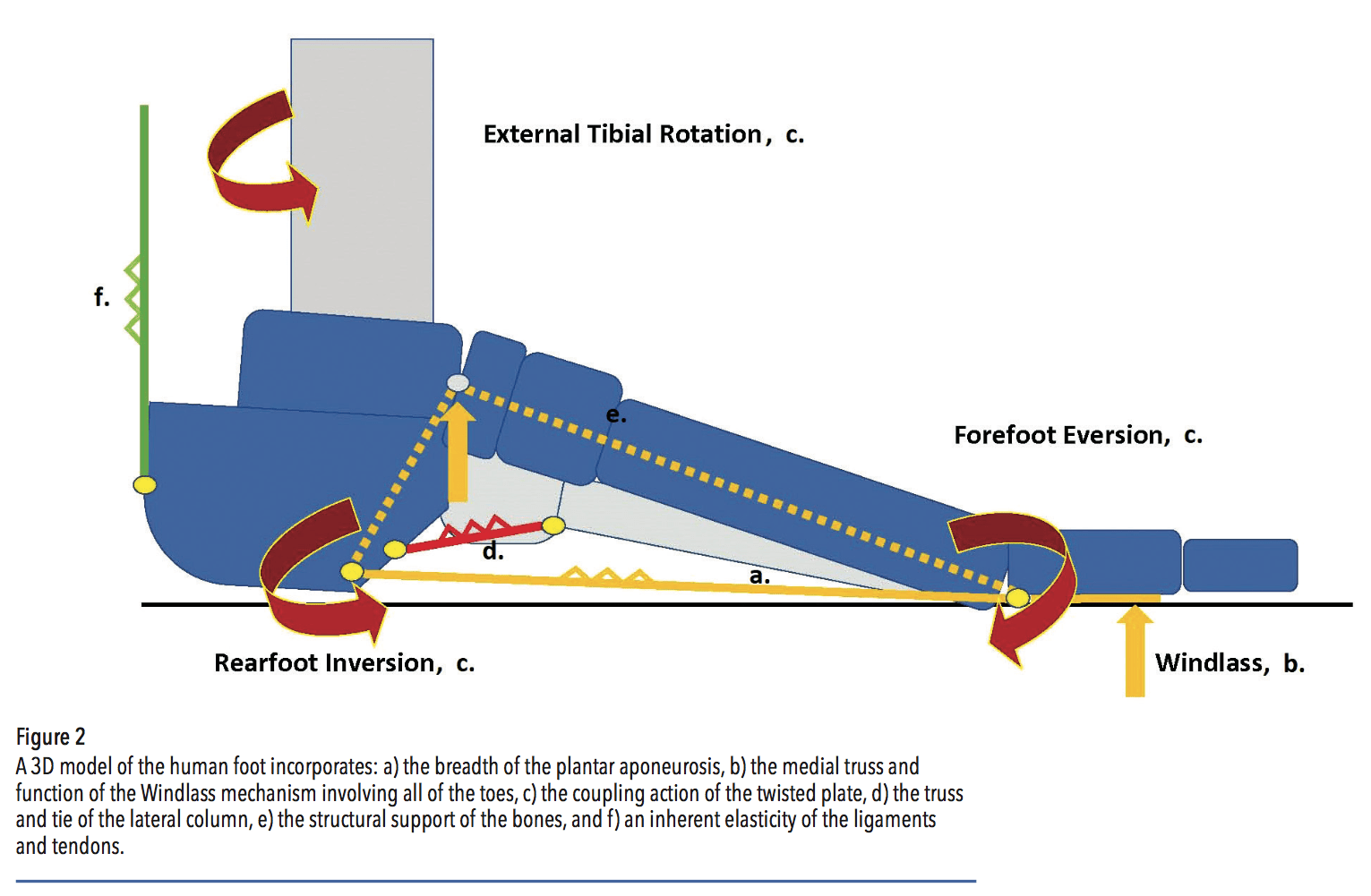
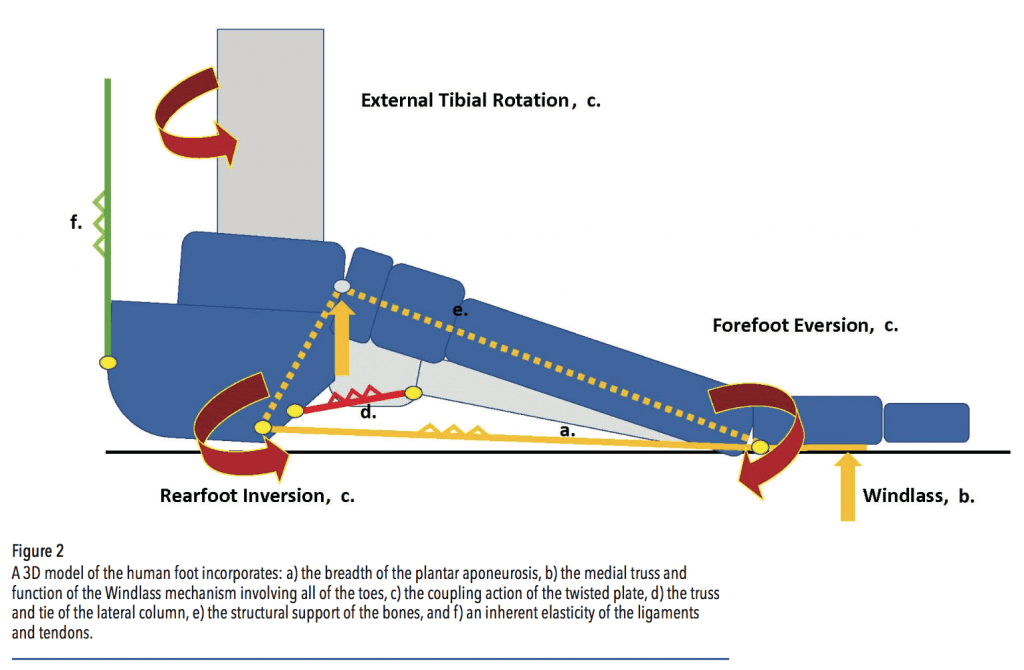
In stance, the plantar fascia acts as a tie or line that prevents the foot from elongating and the arch from collapsing. Several cadaver studies that sectioned or cut the plantar fascia demonstrated it provides approximately one-quarter of arch stiffness and stability. In dynamic gait its function changes. The insertions of the fascia distal to the metatarsal heads facilitate the Windlass mechanism. After midstance when heel rise begins, although plantigrade, the hallux and toes are dorsiflexing on the pivoting foot, and in normal gait the foot begins to resupinate. With unobstructed motion, and enhanced by the sesamoid apparatus, the big toe acts as a crank pulling the fascia taut around the drum of the first metatarsal phalangeal joint (MTPJ). The bones of the midfoot become close- packed and capable of supporting body weight as the foot prepares for swing.
This simple and effective model portrays the Windlass as a two-dimensional truss and tie-rod. In reality, foot function is far more complicated. For example, the Windlass effect is not isolated only to the first MTPJ. Although the medial aspect of the foot undergoes greater deformation and takes more of the strain, dorsiflexion of all the toes disperses the tension laterally. Normal stressing of the plantar fascia during fast walking and running can approach 80 percent of the load-to-failure so it must work synergistically with many other structures in the foot and ankle to share these strains and avoid breakdown.
One such mechanism is the lateral column of the foot, which is supported by a similar, albeit shorter truss. The long plantar ligament originates from the calcaneus and inserts into the cuboid and the bases of the second, third, and fourth metatarsals. Loading the lateral column can distribute and reduce strain in the medial column and the plantar fascia. Other examples of how the arch resists deforming forces and prevents foot injury include the keystone configuration of the midfoot bones, plus the inherent elasticity in the plantar fascia, tendons, and ligaments.
The Twisted Plate Model
The idea of the foot as a twisted plate was originally proposed by MacConaill in 1945 and subsequently developed by Saraffian.1,2 This concept recognizes the forefoot, toes, and metatarsal heads lie flat against the ground—horizontal. But as you move more proximally, the medial metatarsals elevate, the plane twists, and in the rearfoot, the talus sits on top of the calcaneus—vertical. Unlike the hand, all the bones of a normal foot do not rest on a flat surface. This is an adaptation from our primate ancestors. The evolution of an arch in the foot allowed humans to develop efficient bipedal gait. As a consequence, when the rearfoot pronates relative to the stable, flat forefoot, it is actually untwisting. Likewise, rearfoot supination is twisting the foot making the arch higher and more stable. This occurs naturally during each step with the arch height lowering and rising depending on the phase of gait.
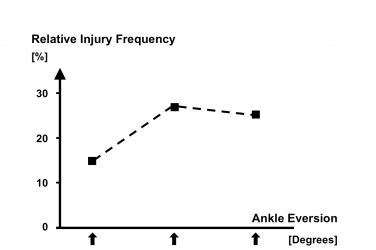
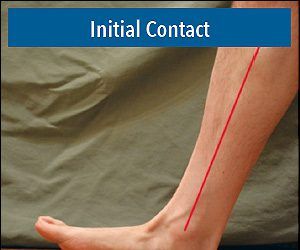
There is a well-defined coupling relationship between tibial axial rotation and foot inversion and eversion. Pronation and supination involve foot motion in all three planes, and they are linked to internal and external rotation of the tibia respectively. It is important to realize that as the foot resupinates after midstance, it is the rearfoot that inverts. The forefoot remains stable on the supporting surface, so it is actually pronating in relation to the rearfoot. Understanding the concept of the twisted plate clarifies that the apex of the foot arch will rise when the rearfoot inverts and the forefoot everts or pronates relative to it. This action accords with the Windlass, and one of the functions of the midtarsal joint is to allow the opposing motion.
Although not intuitive, it means pronation of the forefoot relative to an inverted rearfoot actually lessens tension in the aponeurosis. This conclusion of the twisted plate model was confirmed in a series of studies by Kogler et al.3 Cadaver feet were positioned on a loading frame, and a strain transducer was imbedded into the central band of the plantar fascia. It was noted that placing medial wedges under the forefoot significantly increased strain in the plantar aponeurosis, but lateral wedges decreased it. This was a controversial finding and contrary to accepted belief at the time. It suggests orthotics with forefoot lateral posting reduce strain on the plantar fascia. Interestingly, in the same experiment both medial and lateral wedges placed under the calcaneus had limited influence on plantar fascial strain.
The researchers proposed that the effect of forefoot lateral wedging is the result of two separate mechanisms. Firstly, by pronating the forefoot on the rearfoot, the calcaneocuboid joint is locking, and the lateral column of the foot becomes stable for terminal stance. Secondly, adding support under the lateral forefoot transfers ground reaction force away from the medial side. To underscore this point: Medial forefoot posting on a foot orthotic would increase ground reaction force under the medial column, potentially dorsiflexing the first ray and increasing strain in the plantar fascia.
Orthotics and Footwear
In the last decade the term plantar fasciitis, indicating an inflammation, has come into question. It is now believed it is not simply traction on the fascia but also shearing, bending, and compression that are responsible for developing pain. With an understanding of the mechanics of the arch, orthotics and footwear can be designed to complement plantar fascia operation and limit its strain. Functional orthotics with deep heel cups, medial posts, and medial heel skives can help position the rearfoot for resupination in terminal stance.
Forefoot medial posts should be avoided for several reasons. They supinate the forefoot, working in opposition to the twisted plate model, inducing strain on the plantar fascia. They also place extra force under the first MTPJ, causing a dorsiflexion moment on the distal truss of the first ray. Even worse, if this creates a functional hallux limitus, the effectiveness of the Windlass will be compromised. Conversely, providing a first ray cut-out or a reverse Morton’s extension can potentially enhance motion of the first MTPJ. In cases of equinus, where ankle dorsiflexion is limited, a heel lift can reduce tension in the Achilles tendon thereby easing strain on the plantar fascia.
Shoe gear is another important consideration. Flat soles with zero drop from heel to ball put extra strain on the Achilles and other structures of the foot. Having a shoe with a mildly elevated heel (10-12mm) reduces this. Shoes with contoured midsoles help support and stabilize the lateral column, sharing the loads and forces acting on the medial arch. Stiff soles should be avoided as they inhibit toe dorsiflexion and limit the effect of the Windlass. Physical therapy targeting the action of the toe flexors and strengthening the intrinsic muscles also helps alleviate the symptoms of plantar fasciitis.
Summary
The arch of the human foot is a full three-dimensional support system, and the plantar aponeurosis is vital to its function. The plantar fascia acts as the medial tie in the truss of the Windlass, but it also depends on the strength and dorsiflexion action of the lesser digits to withstand excessive strain. It avoids injury by sharing loads with other mechanisms including the osseous configuration of the foot bones. The lateral arch, supported by the long plantar ligament, is critical to lateral column stability. Finally, the elastic nature of the fascia and multiple other ligaments and tendons act as a web to help distribute load evenly.
For a more complete description of these concepts, see Pathomechanics of Common Foot Disorders, Chapter 8: Plantar Heel Pain, Douglas H. Richie Jr., Springer 2021.
Séamus Kennedy, BEng (Mech), CPed, is president and co-owner of Hersco Ortho Labs, New York. He can be contacted via e-mail at seamus@hersco.com or by visiting www.hersco.com.
References
1. MacConaill, M. .A. The Postural Mechanism of the Human Foot. Proceedings of the Royal Irish Academy 1944-1945 50B:265-78.
2. Sarrafian, S. K. 1987. Functional Characteristics of the Foot and Plantar Aponeurosis under Tibiotalar Loading. Foot Ankle 8:4-18.
3. Kogler, G. F., F. B. Veer, S. E. Solomonidis, and J. P. Paul. 1999. The influence of medial and lateral placement of orthotic wedges on loading of the plantar aponeuro- sis. Journal of Bone and Joint Surg-American Volume 81(10):1403-13.