The journey of a thousand miles begins with a single step. – Lao Tzu
One approach to understanding foot pathology is to appreciate the symphony that plays with each step in human locomotion. The act of walking is a wonderful choreography that is dependent on an intricate interplay of forces and motions across multiple joints. It is a worthwhile field of study. Once the main concepts are grasped, it becomes easier to recognize gait abnormalities that may be the cause of discomfort or pain in a patient. Observed deviations from “normal” gait can be used as a basis for treatment that includes the use of orthotic and pedorthic solutions to alter the timing of key events or restore symmetry. Interestingly, although each individual displays his or her own peculiarities of gait, these average out in clinical studies.
The simplest distinction in gait is between stance and swing. Stance refers to the time the foot is in contact with the ground, and swing is when the foot is in the air for limb advancement. In the classic Gait Analysis: Normal and Pathological Function, by Jacquelin Perry, MD, ScD, and Judith Burnfield, PhD, PT, stance constitutes 62 percent of the gait cycle and swing the remaining 38 percent, at the customary walking speed of 82 m/min.1 Although the percentages and labels vary across different texts, the sequence and stages of gait are the same. As walking is bipedal and body weight is transferred between each limb, stance can be divided further into times when both feet are touching the ground, called double stance, or when only one foot is touching the ground, termed single-limb support (SLS).

Phases of the Gait Cycle




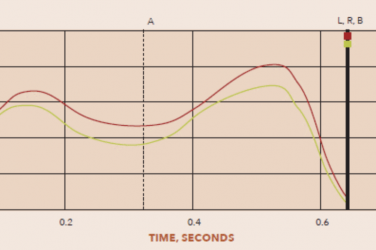
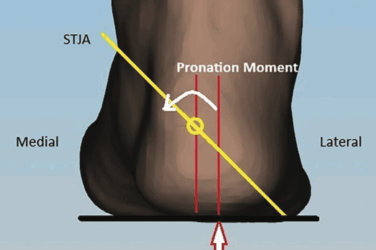
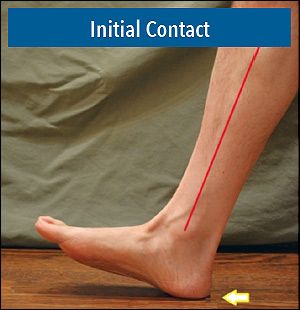
Consider a single stride by following the action of the right foot, beginning when the right heel first contacts the ground. This instance is called heel contact or initial contact, and the trailing left foot is still touching the ground. The left foot maintains contact up to the first 12 percent of the gait cycle as the right foot rapidly goes through loading response. This is the critical early stage of gait at which time the right foot prepares to accept full body weight before the left foot leaves the ground. There is a steep increase in the ground reaction force (GRF) and a sudden transformation in the orientation of the subtalar joint (STJ) into eversion.
Perry and Burnfield developed the idea of four “foot rockers” associated with the period of stance. The heel rocker acts from initial contact through loading response and makes up the first 12 percent of the gait cycle. The term “heel rocker” may be somewhat of a misnomer as it is the momentum of the body and the synergistic action of the lower-limb muscles that ensure the foot proceeds to make full contact with the supporting surface. After heel strike, the tibialis anterior and other ankle dorsiflexors act to decelerate the foot as it moves toward the ground in a controlled manner. However, the concept of a pivot at the heel is valid, especially in a rehabilitation setting, when the natural action of the ankle joint has been inhibited. Examples include the effects of ankle arthrodesis or the provision of a solid-ankle AFO. In cases where the ankle is rigid, it may help to provide a posterior rocker, such as a negative heel on an orthopedic shoe. This technique is sometimes used in prosthetics by fitting the patient with a SACH foot, which provides better shock absorption and a more beveled interface with the ground.
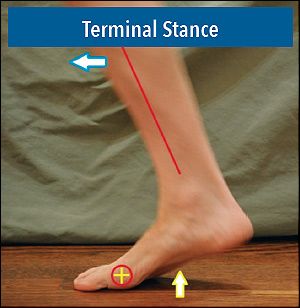
SLS comprises the next 38 percent of the gait cycle, divided into mid stance and terminal stance. In mid stance (12 to 31 percent of the gait cycle), the foot is flat on the ground supporting the body as the tibia accelerates past vertical. The fixed foot must absorb all forces and simultaneously allow the forward movement of the center of pressure (COP) to the metatarsal heads. Fluid progression through SLS depends on many factors including the uninterrupted action of the ankle joint, or ankle rocker. Midway through SLS, the heel begins to rise, marking the transition to terminal stance (31 to 50 percent of the gait cycle). Body weight now falls beyond the area of foot support, and the hinge action of the metatarsals constitutes the forefoot rocker.
The final component of stance occurs with the left foot reestablishing initial contact and the right foot now in pre-swing (50 to 62 percent of the gait cycle). This second instance of double stance provides momentary stability as the right foot prepares for swing. Throughout the stance period, there is a migration of the COP moving distally through the foot and from lateral to medial. As a mobile adaptor, the foot needs to provide stability while allowing this smooth forward progression. The final toe rocker relies on the medial forefoot and hallux. The left foot then accepts full body weight as the right foot propels off the ground. It is important to appreciate that disruption or limitation in any of the phases breaks the flow and timing of the entire sequence.
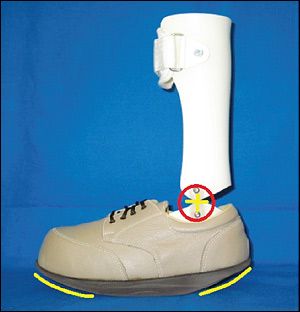
This view of gait considers motion in the sagittal plane, and certainly the largest range of motion (ROM) of the hip, knee, and ankle occurs in that plane. When working with patients with amputations or gross motor dysfunctions, providing stability and restoring function in the sagittal plane are often the primary objectives of the practitioner for providing an orthotic or prosthetic device. AFOs, CROWs, and other braces are frequently prescribed to limit motion due to muscle weakness or to prevent further joint or tissue damage. With careful design, it may be possible to replace lost joint motion. For example, AFOs with full-length, rigid foot plates that limit flexion at the metatarsal heads can be augmented with forefoot rocker soles.
The goal when designing and dispensing orthotic devices is always to restrict painful or damaging motion without blocking beneficial motion. Posterior leaf spring (PLS) AFOs can prevent foot drop and toe drag yet still permit the tibia to somewhat dorsiflex on the plantigrade foot. Likewise, flexible hinged ankle joints such as those manufactured by Tamarack Habilitation Technologies, Blaine, Minnesota, retard motion in the transverse plane without fully blocking it. Within each stride, there is a synergy of motion occurring in all three planes that needs to be maintained if aspects of normal gait are to be preserved.
In Part II of this series, we will go beyond the sagittal plane and consider the crucial role of frontal plane motion below the ankle and the significance of pronation in human walking.
The author gratefully acknowledges the help and contribution of Paul R. Scherer, DPM, MS, clinical professor at Western University School of Health Sciences, College of Podiatric Medicine, and founder of ProLab Orthotics, Napa, California.
References
- Perry, J., and J. Burnfield. 2010. Gait Analysis: Normal and Pathological Function, 2nd ed. Thorofare, NJ, Slack Incorporated.