The most widely taught and accepted theory of foot biomechanics was developed by Merton Root, DPM, and his colleagues during the second half of the 20th century. Root’s studies were instrumental in creating the modern foot orthotic industry and represented a quantum leap forward from prior thinking. At its heart, Root’s theory is based on the position of the subtalar joint (STJ) and the midtarsal joint (MTJ), and their relationship to the forefoot. Determining the relative angulation between a neutral rearfoot and a maximally pronated forefoot was considered of elemental importance to understanding foot mechanics and often predictive of pathology. (For a fuller discussion, read “An Overview of (Early) Foot Orthotic Biomechanics, Part I“ )
Later research gave rise to the tissue-stress approach, which enhanced the model of the functioning foot. Tissue-stress looks at all of the forces acting on the weight bearing foot-rather than just joint position or motion. The location of the ground reaction force (GRF) and the subsequent rotational moment of the foot about the STJ axis determine the net force and the resulting pathology. (Author’s note: For a fuller discussion, read “Foot Orthotic Biomechanics, Part II)
 Long axis of the foot is at a right angle with the long axis of the body.
Long axis of the foot is at a right angle with the long axis of the body.
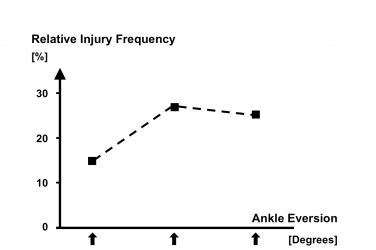
While these theories differ in approach, they do share one common factor: they primarily consider the foot in the frontal plane. The body has three cardinal planes: frontal (as seen from the front), transverse (as seen from above), and sagittal (as seen from the side). Many body motions occur in all three planes, and foot motion is no exception. Pronation, for example, describes tri-planar motion involving eversion (frontal), abduction (transverse), and dorsiflexion (sagittal). Thus, a full understanding of foot and ankle motion requires consideration of tri-planar motion (figure 1).
The Windlass Mechanism in the Sagittal Plane
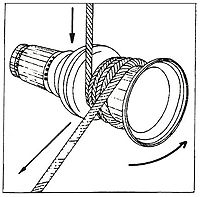
Generally speaking, a windlass is a cable wound around a revolving drum. An everyday example of a windlass is a winch used to hold tension on a sail (figure 2). In the 1950s, J. H. Hicks described the windlass mechanism of the foot. In examining the foot in the sagittal plane, he noted that it displayed similar characteristics to a windlass. The medial plantar fascia (PF) “winds around” the first metatarsophalangeal joint (MPJ) during hallux dorsiflexion. This causes an elevation of the medial arch of the foot and a passive resupination.
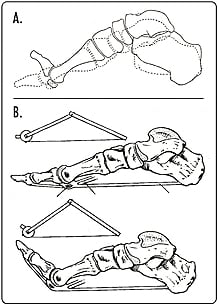
The effect is most clear if the medial foot is modeled as a truss (figure 3). Simply speaking, a truss is a triangular architectural support consisting of hinged “members” connected by a tie or rod. Shortening the tie along the base will raise the apex of the triangle. Hicks noted that the following effects occur simultaneously during passive first MPJ dorsiflexion:
- An increase in medial longitudinal arch height.
- Inversion of the rearfoot (as the PF draws the calcaneus anteriorally).
- External rotation of the tibia.
- Appearance of a tight band in the PF region.
Dorsiflexion of the first MPJ has the effect of shortening the PF and pulling it taut. Much like a hinged truss, this automatically raises the arch of the foot. At the same time, the bones become close-packed. This stabilizes the moving foot and converts it from a flexible adapter (necessary in the early phase of gait) to a rigid lever (which is essential for the propulsive phase of gait). For example, in stair climbing the foot remains a rigid lever as the forefoot dorsiflexes on each step. Studies on cadavers and patients with paralysis show that this is a mechanical effect that is dependent on unrestricted range of motion (ROM) of the first MPJ and is not muscle dependent.
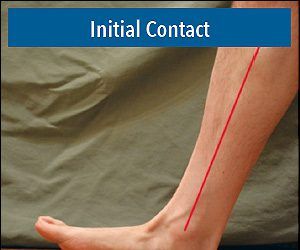
A simple test for the windlass effect is called the Hubscher maneuver. It entails passive dorsiflexion of the first MPJ. You should observe an increase in arch height and the emergence of the PF band. A normal healthy foot will exhibit approximately 80 degrees, plus or minus, of dorsiflexion at the first MPJ, depending on ankle position. The windlass mechanism starts at mid stance, as propulsion begins, and counteracts pronation.
Loss of this mechanism leaves the bones of the foot “loose” during critical third rocker, and there are many diagnoses that limit the motion of the first MPJ. Conditions such as hallux rigidus, functional hallux limitus, and severe pes planovalgus restrict the operation of the windlass mechanism, and hallux amputations obviously disrupt the effect. In such cases, patients will often present with a more everted gait as the foot fails to resupinate.
In designing orthotics and shoes, practitioners should be mindful not to restrict first MPJ motion. There is a trade-off between stiff-soled shoes and foot function. Firm rocker soles, sole stiffeners, AFOs with full-length foot plates, and the current mainstream trend in roller-soled toning shoes will reduce first MPJ dorsiflexion. To encourage the effect, orthotics can be designed that help plantarflex the first metatarsal bone by raising the arch and still allowing for full first MPJ dorsiflexion. Orthotic modifications such as first ray cutouts and kinetic wedges can be used to enhance the windlass mechanism.
Transverse Plane Mechanics
Much of the early work on the foot was done in open-chain. Evaluation of joint ROM, measurement of rearfoot to forefoot relative position, and plaster casting were regularly performed non-weight bearing and static. While foot orthotics are often prescribed to address frontal plane mechanics such as STJ motion or calcaneal eversion, the exact mechanisms by which they work are still open to debate.
When we ambulate, the foot functions dynamically in closed-chain. Close examination of the foot and lower leg during walking and running reveals that a complex series of events occur with each stride. Over the years, work on both cadavers and human motion studies in biomechanics labs have revealed the intricate kinetic relationship between the foot and leg under load.
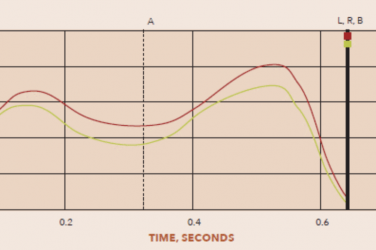
One study in the Journal of Orthopaedic and Sports Physical Therapy (JOSPT), “The Effect of Foot Orthotics on Three-Dimensional Kinematics of the Leg and Rearfoot During Running” (1995;21(6):317-327), involving a group of 20 recreational runners, looked at the effect of using semi-rigid foot orthotics on three-dimensional kinematics. Researchers noted that wearing orthotics had a significant effect “in the coupling relationship between tibial axial rotation and calcaneal inversion/eversion;” i.e., a frontal plane modality had a significant effect on transverse plane motion. Even more noteworthy: “No differences were found for the frontal plane rotations for either group [low or high rearfoot profile] when orthotics were worn.” The findings suggest that the maximum effect of orthotics is realized within the first 50 percent of stance and related to changes in tibial axial rotation.
In another study published in JOSPT, “Transverse-Plane Mechanics at the Knee and Tibia in Runners With and Without a History of Achilles Tendonopathy” (2008;38(12):761-767), researchers evaluated a group of 16 runners-eight had a history of Achilles tendonopathy (AT) and eight were in a non-injured control group. The examiners looked specifically at transverse plane motion and moment at the knee and distal tibia. They found that “runners with a history of AT exhibited less internal rotation at the knee and less external rotation moment at the tibia,” concluding that “transverse plane motion and control during running may have implications for function in other planes.” This raises the interesting point that although the AT and gastroc-soleus muscle group work primarily in the sagittal plane, slight variations in motion in the other planes may be contributing to injury.
These studies, among others, reinforce the idea that walking and running are tri-planar activities and that it is not obvious which plane is responsible for a presenting pathology. We should always consider the effects of our devices in all three planes-knowing that altering one will manifest changes in all. Medical evidence strongly indicates that the majority of symptomatic runners who wear foot orthotics show improvement. This includes injuries above the ankle such as patellofemoral pain and iliotibial band syndrome. As a profession, we need to continue to develop our understanding of the interconnectedness of the foot and leg in motion and then use that knowledge to enhance the orthotic designs that so clearly benefit our patients.