Billions of pairs of shoes are sold annually in the United States. Human anatomy, although clinically standardized, is certainly unique from individual to individual. Given both of these statements, it is no surprise that much of the footwear bought today may not be a perfect fit for the wearer.
Fortunately, there are many and varied ways that shoe fit can be optimized. Pedorthists dedicate themselves to the study, fitting, and modifying of footwear and foot orthotics in order to give the wearer the ideal shoe function. Changes can be made internally, externally, or a combination of both.
External Pedorthic Shoe Modifications
When shoe modifications are applied correctly, or used in conjunction with foot orthotics, the results can be quite remarkable: aiding in the transfer of forces; off-loading at-risk or sensitive areas of the foot; rebalancing or realigning the musculoskeletal system; accommodating fixed deformities; and controlling motion.
Modifying Off-the-Shelf Footwear: Advantages
There are many obvious advantages in being able to modify off-the-shelf footwear. Whether the shoes are fashionable or extra-depth, patients like that “factory-made” look. Working with their store-bought shoes allows them to control, to some degree, the style, color, and shape of the shoe. These shoes also are less expensive than custom-made shoes and perhaps will allow for some variety over time.
Unlike foot orthotics, which can be transferred easily, shoe modifications, either external or internal, become a permanent aspect of a particular shoe and make it expensive to modify every shoe. This may restrict the wearer to a single pair, which is never an ideal situation. In addition, external adjustments may wear down quite quickly and lose much of their efficacy, requiring constant vigilance and refurbishment. The following are some of the more commonly applied modifications. In the descriptions I have included some of the possible Therapeutic Shoe Bill (TSB) A-Codes and HCPCS L-Codes, although this list is by no means complete and should only serve as a guideline for further investigation.
Flares: If ever you ascend a public staircase, as I do daily in the subway system of New York City, and observe the person in front of you, you can quickly tell if he or she rolls in or out on the shoes. Pronation and supination are readily obvious. Usually if the eversion or inversion is pronounced, the entire shoe will have broken down on one side. The sole may be much worn, the upper may be stretched and sagging over the welt, and the counter may have broken down. There are several adjustments that can be made to correct or control such a foot.
 |
| Heel and sole elevation with flares. |
The mildest change is to add a flare to the sole of the shoe. A flare is an extension of the base of the shoe, below the welt, medially or laterally. Usually a flare has a beveled edge. It may be at the heel only, under the sole only, or it may run the full length of the shoe. It widens the shoe, resisting rotation, making it more difficult for the wearer to roll out on that side. It does not attempt to correct the problem, just to impede it.
Flares also have the advantage of making shoes more stable. Patients who present with balance issues may well benefit from having both medial and lateral flares applied to their shoes. Although the shoes may look a little clunky, this will provide a wider base for them to stand on. Flares also are known as “off-set heels;” this is the term used in the Medicare diabetic TSB, Code A-5506. (HCPCS L-3390)
Wedges: If the foot is flexible and some correction is desired, an external wedge can be applied to the shoe. Medial or lateral heel wedges add an extrinsic posting to the sole of the shoe to promote heel varus or heel valgus respectively. Once again wedges can be at the heel, the sole, or applied heel to sole. In a case where the patient presents with a fixed deformity, wedges can be used to accommodate the position of function, bringing the ground up to the foot. Wedges are covered in the TSB under Code A-5504. (HCPCS L-3350, L-3360, L-3370, L-3380, L-3420)
External counters: A more aggressive shoe adjustment to provide motion control is the addition of an external counter. This also is known as a “buttress,” a “stabilizer,” or an “outrigger.” External counters are made by layering firm neoprene or crepe (Durometer >55) from the ground to up above the welt and onto the quarter of the shoe. The effect is to fully support the foot and ankle, provide a wider base, and reduce flexing. This is best used when the patient presents with a fixed deformity, such as an equinovarus clubfoot, and the patient will benefit from fairly rigid support. External counters are not aesthetically attractive, so I recommend only using them as an option of last resort.
Cushion heels: A cushion heel is often referred to as a SACH heel (solid ankle cushion heel). This is simply the replacement of a triangular wedge, taken from the heel, with a lower durometer sponge rubber. This allows the heel of the shoe to compress at heel strike and absorbs some of the impact forces. (HCPCS L-3340, L-3450)
Elevations: Shoe lifts to accommodate leg-length discrepancies are probably the most common adjustments seen on regular shoes. This topic was discussed more fully in an article in the August 2005 edition of The O&P EDGE.. (HCPCS L-3300, L-3310, L-3320, L-3334)
 |
| Forefoot rocker sole with slight negative heel |
Rockers: There are a number of techniques to transfer and offload plantar pressure and improve gait. Rocker soles reduce energy consumption as they propel the body forward after the center of gravity has passed over the apex of the rocker. Rockers also can help patients with limited ranges of motion at the ankle or metatarsophalangeal (MTP) joints.
Rockers are created by adding extra crepe to the midsole portion of the shoe and then beveling it away just proximal to the point of pressure. Some rockers have a rock at the forefoot only, and others rock at the anterior and posterior ends of the shoe; all have a flat stable area at mid-stance. Rockers are listed in the TSB under code A-5503. There are many styles and types of rocker named in the pedorthic and orthotic literature, the following list only indicates the main categories.
Forefoot rockers–Reduce ground reactive forces to the metatarsal heads, inhibit demand for dorsiflexion at the MTP joints and assist at toe off. These are good for patients with met head problems such as metatarsalgia and hallux rigidus or those with forefoot lesions or ulcerations.
Rearfoot rockers–Lessen the demand for motion in the ankle joint and reduce impact at heel strike.
Roller sole–This sole has no flat spot in the midfoot. There is a gentle curve from heel to toe. It allows the patient to roll through from delayed heel strike to toe off. This sole modification is similar to that of a CROW boot or CAM walker. Used in conjunction with a sole stiffener, this will prevent any flexion of the foot, but some patients may find it unstable.
 |
| Metatarsal bar. |
Metatarsal bars: Much like rocker soles the general term “met bars” refers to a whole family of specific shoe modifications, each with unique names: Jones, Thomas, Crescent, Mayo, Denver, etc. All met bars are designed to help metatarsalgia and relieve plantar pressure by adding a wedge of firm material across the sole of the shoe just proximal to the met heads. This unloads the pressure from the met heads, allowing for rapid transfer from the shafts of the metatarsals to the distal end of the toes, with limited extension of the digits.
Met bars are typically ¼” in vertical height, which can make them a tripping hazard. They can be made using firm crepe or leather. Unlike rockers, met bars have a much flatter plantar surface, providing a broader area of contact with the ground. Met bars are included in the TSB under code A-5505. (HCPCS L-3400, L-3410)
 |
| Spring steel sole stiffeners |
Stiffeners: Sole stiffeners can be added to almost any shoe to limit flexion. They are usually made from spring steel or carbon fiber, and they run from mid-heel to forefoot.
They are added to the midsole of the shoe, layered between the innersole board and the outsole.
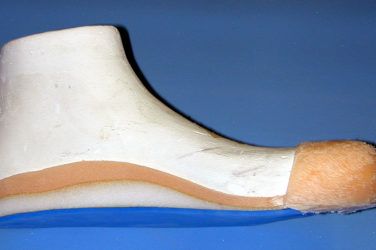
Stiffeners are useful for treating patients with conditions such as stress fractures, hallux rigidus, and MTP joint arthritis. Stiffeners are often applied in conjunction with one of the rocker options so as not to totally restrict motion. They also are helpful for trans-met amputees using a partial foot prosthesis when you want to protect the distal foot from impacting the toe filler.
 |
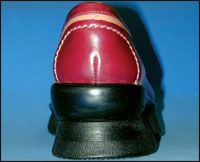
| Toe guard. |
Toe guards: Patients with peripheral neuropathy often require shoes with softer, more pliable uppers. However, they may operate in harsh environments that will quickly cause the toe box to deteriorate. Examples include at-risk diabetics working in industry or those engaged in outdoor activities. Toe guards, also known as “bumper guards,” are the addition of a harder plastic or coating onto the front portion of the shoe to prevent it wearing down too quickly.
These are some of the many and varied external pedorthic shoe alterations that are possible. They can be used separately or in conjunction with one another. The shoe is the final building block upon which orthotic therapies or even surgical procedures will rest. Optimizing fit and function with the overall aim to improve patient outcomes is the pedorthist’s mission.
Internal Pedorthic Shoe Modifications
As we all know there are two sides to every story: having considered the outside, it is now time to look at some of the changes that are possible inside a shoe. Much like the marvels of plastic surgery, a little nip here and tuck there can optimize the feel and fit of a shoe without having to compromise the outward appearance.
 |
| Heel spur excavation with PPT plug. |
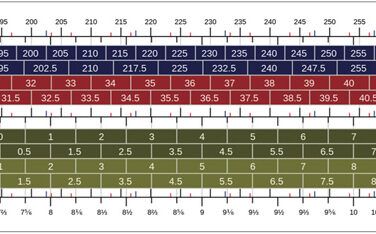
There is never a bad time to take the pedorthic high ground, so the first consideration for footwear is to ensure that it is properly sized in both length and width. If there is not adequate room inside the shoe, the addition of internal modifications may only cramp and worsen the situation. The shoe is the platform upon which any modifications rest; having firm counters, long-laced eyestays and a sensible heel height (1/2 in. to 1 in.) will form the best foundation to control the foot.
The advantages of internal modifications are that they are frequently less expensive, and they are usually easily replaced if they become worn. They also come into direct contact with the foot, acting at the site of concern. Internal modifications typically will not wear down as quickly as external modifications. However, unlike custom foot orthotics, they often are not transferable, so you may need to apply one in each pair of shoes, possibly limiting the footwear available to a patient. In addition, they may reduce the shoe volume, leading to an unexpected fit issue.
Some of the more popular internal shoe modifications are discussed below.
Heel cushions: One of the simplest changes to make to a shoe is to insert a heel cushion. Cushions have been shown to relieve mild cases of plantar fasciitis or early heel pain syndrome. Cushions can be made from a wide variety of materials of various durometers. Foams, sponge rubbers and silicone all are possibilities. Heel cushions can be effective on two fronts: providing shock absorption to a sensitive part of the foot and acting as a slight, albeit compressible, heel raise.
Heel elevations: Shoe lifts to accommodate leg-length discrepancies are probably the most common adjustments seen on regular shoes. Internal heel lifts are made from firm cork or neoprene. This topic was discussed more fully in the article from the August 2005 edition of The O&P EDGE’s “Stepping Out” department.
 |
| Left: Cork Barton’s wedge. Center and right: Rubber heel wedges. |
Heel wedges: A mild correction for a pronated foot displaying heel valgus is the insertion of a “pear” shaped wedge under the medial heel. You can add up to 3/8 in. of firm material, either a crepe or leather, and skive the distal edges to zero. This is similar to adding extrinsic posting to a foot orthotic. For supinators with heel varus, the wedge should be placed on the lateral side. A Barton’s wedge is longer and extends from the heel to just behind the met head on the effected side.
Metatarsal pads: The addition of metatarsal pads onto the shoe insole will help alleviate the symptoms of metatarsalgia by building a met arch, and transferring some of the weight bearing pressure from the met heads unto the met shafts. Met pads come in many different sizes, heights, and materials ranging from spongy PPT and felt to harder orthopedic rubbers. Patients with neuromas will only benefit from met pads as long as the shoe has enough volume to accommodate the foot plus the pad!
The main difficulty for the practitioner is being able to place the pad correctly inside the shoe. It is best to make a trial fit with a self-adhesive pad or make a transfer mark using lipstick before permanently bonding the final pad in place.
For patients that require broad metatarsal relief, met bars can be placed under all five met heads. Likewise sesamoid pads allow a drop for the first met head and transfer pressure laterally by raising the second, third, and fourth.
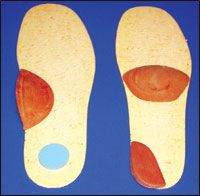 |
| Left: Scaphoid pad and heel plug. Right: Met bar and heel wedge. |
Schaphoid pads: These pads also are known as longitudinal arch pads and used to be referred to as cookies; they were quite popular in times past. Scaphoid pads can be made from a variety of materials, firm or soft rubbers or even leather. They are cemented into the shoe at the medial arch, giving extra support under the midfoot. When a shoe is too narrow in the shank to accommodate a foot orthotic, they often are the only alternative for providing some support.
Excavations: These refer to any depressions or cutouts created to the inlay or insole to reduce pressure in a localized area. For example, patients presenting with a calcaneal spur may benefit from a round plug being removed from the central aspect of the heel. This then can be filled in with a compressible PPT or viscoelastic type material.
Stretching: One of the simplest adjustments to make to any shoe is to stretch it. Shoes can be stretched in both length and width if necessary, adding slightly more volume. However, there are limits to what can be achieved as the innersole board does not stretch, and the shoe upper may begin to look swollen. There are a number of stretching systems available on the market from simple manual shoe-tree type units to heated shoe racks. You will get the best results when using a shoe stretching liquid, which can be purchased from any shoe finder wholesaler.
Localized stretching can be achieved with the use of a Ball and Ring device. These are excellent for creating a mound or bump at a particular spot on the upper. Although seldom pretty, they can give significant relief for patients with bunions or severe hammertoes.
Carbon plates: Patients with met head fractures, hallux limitus, or turf toe often require restricted range of motion at the met heads. The insertion of a carbon footplate into a shoe will limit flexion. This is a good alternative to cementing a permanent steel shank into the shoe’s midsole as the plate is both transferable and eventually removable. The thin plates are low bulk and lightweight and they can be used in conjunction with custom foot orthotics when necessary. They also have a beneficial energy return component when the plate springs back into shape at toe off.
There are many other changes that can be made to shoes such as: relasting to accommodate extra-wide feet; conversions from lace to Velcro closures; additions of firmer counter materials, etc. Some of these techniques have been in use in the pedorthic field for more than 100 years. Skilled shoemakers and cobblers can be quite ingenious in the methods they employ to adjust shoe fit.
However, there has been a tremendous increase in the variety of reasonably priced extra-depth shoes, extra-wide shoes, and shoes with expandable spandex or woven uppers. This market response to the needs of the diabetic and geriatric populations has made some of the more sophisticated shoe adjustment techniques cost-prohibitive. Yet, when used judiciously, internal modifications can significantly alter a shoe’s function without compromising on style.
Séamus Kennedy, BEng (Mech), CPed, FAAOP(A) is president and co-owner of Hersco Ortho Labs, New York, New York. He can be contacted at seamus@hersco.com or by visiting hersco.com.