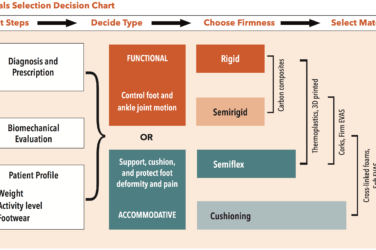


One of the early pioneers of pathology-specific orthotic design was Paul Scherer, DPM, former chair of the Department of Biomechanics at the California College of Podiatric Medicine. In his book Recent Advances in Orthotic Therapy, Scherer outlined this philosophy, describing it as a way to “improve clinical outcomes, promote more consistent research, and advance the acceptance of orthotic therapy as a valued therapeutic modality.”(1) He believed a complete understanding of pathology and foot type should inform orthotic design.
Of course, any prescription guide needs to be interpreted in relation to the actual patient. Firstly, individual anatomy is unique so there are no single sure-fire solutions that work for all. Experience has shown there are always exceptions, and it is important to remain open to these possibilities. Secondly, there is often more than one right answer, and we should appreciate there may be several good treatment options.
Biomechanical Exam
To be successful in dispensing foot orthotics, it is vital to understand the underlying etiology and essential to avoid a tendency toward quick conclusions. Preconceived notions regarding possible causes and potential cures for pedal complaints often obscure the full picture. Conducting a standard biomechanical evaluation is the best way to maintain an open mind. By following a systematic approach, you develop invaluable experience identifying normal and abnormal anatomy. A thorough exam includes gait analysis, a structural biomechanical assessment, testing muscle strength and flexibility, worn-shoe evaluation, recording activity and training level, and noting systemic diseases. Using the same standard form and procedure for each patient makes you less likely to overlook subtle signs that may be present. (“Conducting a Biomechanical Evaluation I & II;” Dec 2017, Feb 2018, The O&P EDGE)
To underscore this point, it is accepted that multiple factors often contribute to a single diagnosis. Richard Blake, DPM, creator of the Blake inverted orthotic technique, uses the “Biomechanical Rule of Five” to remind colleagues there can be up to five distinct factors leading to a specific problem. To put it bluntly: Don’t end your investigation at the first finding. A good example is metatarsalgia. An original paper studied a group of 98 patients that had complaints of pain in the forepart of the foot and isolated 23 separate diagnoses.(2) It was found that 31 of the 98 patients had two or more mechanical etiologies for primary metatarsalgia, and that often primary and secondary metatarsalgia existed together. Despite the same symptom, there are several different orthotic designs to treat this varied patient group. The following are brief descriptions of some of the more common foot and ankle pathologies including outlines for orthotic and pedorthic treatment.
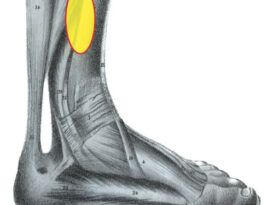
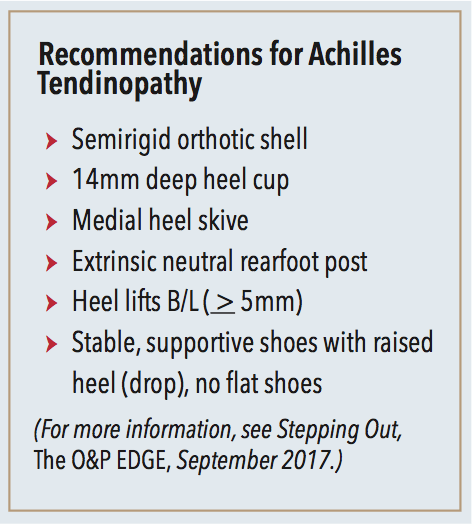
Achilles Tendinopathy
The Achilles tendon is the strongest and largest in the body and is a common site of injury among athletes and weekend warriors. In the literature, Achilles tendinopathy has a reported incidence in runners between 6.5 and 18 percent, but one-third of those diagnosed are sedentary patients.
One of the more common treatments to relieve strain on the tendon is to provide a heel lift. Elevating the heels by 5mm or more may be sufficient to reduce the stretch on the Achilles, and lifts have the added benefit of plantar flexing the foot, increasing the longitudinal arch. Raising the heel naturally lowers tension on the internally twisting tendon. Once the symptoms have been alleviated, it is important to work on the root causes of the problem by improving strength and enhancing biomechanics. Eccentric stretching and strengthening are quite successful in the treatment of Achilles tendinopathy.
Foot orthotics can be designed to alter kinetics and motion, and they have been shown to be effective in an overall treatment plan. Semi-rigid orthotics with deep heel cups and rearfoot extrinsic posts offer control for the foot, limiting eversion and enhancing the timing and duration of pronation. It is easy to incorporate a cork or crepe heel raise onto the orthotic and gradually lower it over time as the tendon heals.
It is also important to wear well-fitting and appropriate shoes that provide stability and support for the foot and orthotic. Flat shoes or flip flops should be avoided.

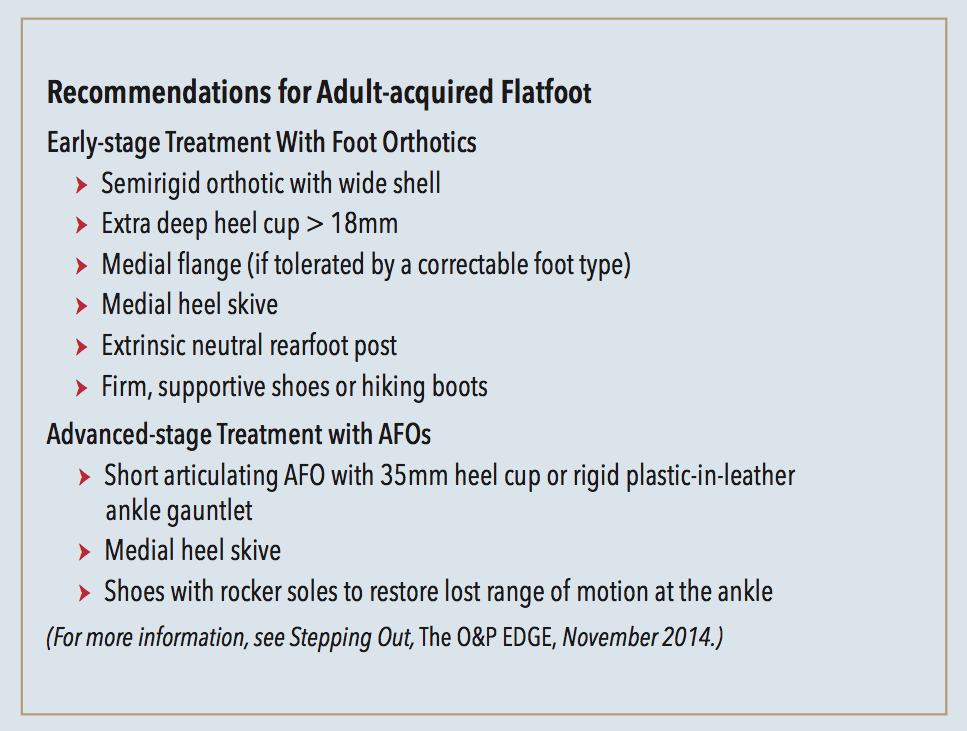
Adult Acquired Flatfoot and PTTD
Adult-acquired flatfoot (AAF) is the term used to describe the progressive deformity of the foot and ankle that over time results in badly deformed and collapsed feet. It is caused by a loss of the dynamic and static support structures of the medial longitudinal arch, and results in an incrementally worsening planovalgus deformity associated with posterior tibial tendonitis. What begins as a predisposition to flat foot can progress to a collapsed arch and then to the more severe posterior tibial tendon dysfunction (PTTD). Each of these are a single step along a broader continuum.
The progression of AAF was originally classified into four distinct stages. Since then, the stages and associated treatment protocols have been further refined, and Stage II has been subdivided into categories A–E. In the early stages, orthotic and pedorthic solutions can address the loss of integrity of the foot’s support structures, potentially retarding further destruction. The treatment should match the stage of deformity and not excessively restrict beneficial motion.
In Stage I, the patient can be prescribed custom foot orthotics and well-fitting shoes. The goal is to support the foot and, if possible, minimize the effects of late-stage pronation. Orthotic modifications such as deep heel cups, medial heel skives, medial flanges, and rearfoot varus posts can all help redirect and alter ground reaction forces. In some cases, requesting a first ray cut-out or reverse Morton’s extension can restore lost motion at the first metatarsophalangeal joint (MPJ), which will enhance the stabilizing effect of the Windlass mechanism. Hiking boots with stiff high counters are recommended to reinforce the medial column and provide support above and below the ankle.
As AAF progresses, foot orthotics may no longer offer sufficient support to control the foot and ankle complex. Early in Stage II, physical therapy to strengthen and rehabilitate the weakened posterior tibial muscle and tendon can be quite beneficial. It often becomes necessary to graduate to an AFO that will control the foot and maintain the coupling of motion across the ankle joint. Short articulating AFOs such as the Richie Brace are well suited to early Stage II treatment. The deep heel cup and high medial and lateral struts enhance the tibial coupling. Patients tend to accept these devices as they can often be worn in sneakers or extra-depth shoes. Using articulating joints at the ankle enables full range of motion in the sagittal plane allowing patients to walk relatively normally. Hinged devices are advantageous as they still recruit regular muscle activity which helps control forefoot abduction.
Later in Stage II and into Stage III it becomes necessary to provide more control. If the midfoot becomes destabilized and forefoot abduction continues, ankle gauntlets such as the Arizona type can be employed. Gauntlets made from rigid polypropylene are much more restrictive and may require a change of footwear to a wider lasted shoe with an open throat. Chukka-style shoes or high-tops are recommended as they provide more support and help keep the AFO properly seated. A rocker sole can be added to the shoe to replace some of the lost motion at the ankle. In more advanced cases where surgery is not possible it may be necessary to consider a solid ankle AFO.

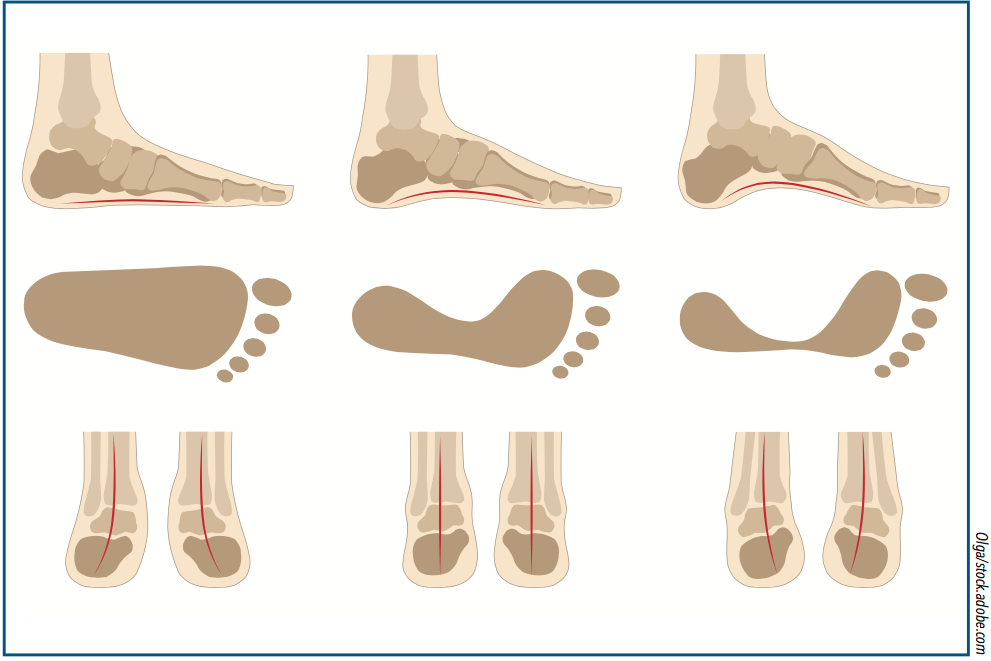
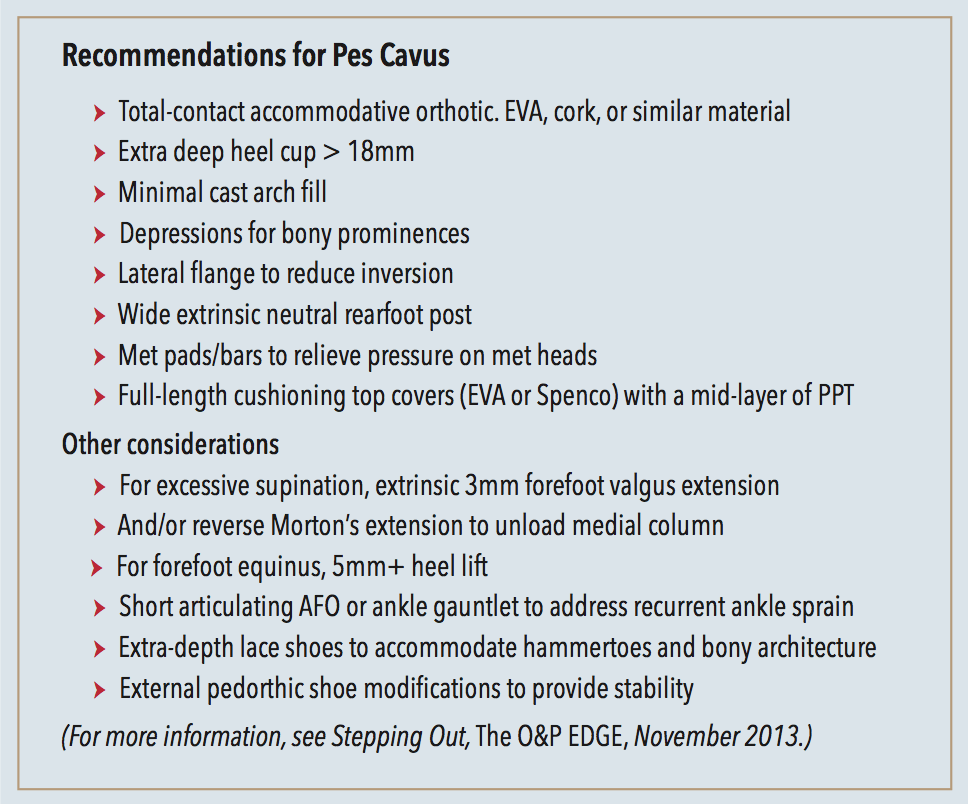
Pes Cavus
Although the estimated incidence of pes cavus within the general population ranges from 8 to 15 percent, a majority of these patients will experience foot pain. Pressure maps sometimes demonstrate the classic tripod characteristic of cavus feet showing a concentration of weight bearing at both the first and fifth metatarsal heads and at the heel. This clear imprint of high pressure also serves as a basis for orthotic treatment. Other indications include the nature of the symptoms typically presented, including metatarsalgia, pain along the lateral column of the foot, lateral ankle instability and recurrent inversion sprains, plantar fasciitis and heel pain, and stress fractures of the lesser metatarsals.
Total-contact accommodative orthotics that cradle the foot and evenly distribute pressure across the entire plantar surface will be beneficial. Softer EVAs and foams can help replace shock absorption that is often lacking, but nonrigid thermoplastic devices that make full contact also work well. Plaster casts should be prepared with minimal arch fill to “bring the ground up to the foot,” and the orthotic should be wide enough to encompass its full width. Depressions or drops relieve specific areas of pressure, which are often indicated by the presence of a callus. Wide, cushioning met pads or met bars will relieve pain and redistribute load away from plantarflexed met heads. Top covers such as Spenco or an underlayer of PPT are also excellent cushion choices.
Posting depends on the primary site contributing to the deformity but should only be prescribed based on the available range of motion. A wide neutral rearfoot post increases the lateral ground reaction force at heel strike. Deep heel cups also help control the tendency toward inversion. Patients with an anterior cavus or forefoot equinus essentially have a downward angled or dropped forefoot which can be offset with a heel raise extending to the mid-arch.
Generally, cavus feet require shoes with plenty of room for a high instep. Many of these feet present with a characteristic bump on the dorsum that is easily irritated by the shoe’s tongue and closure. Blucher-type shoes with padded tongues are often the best choice. There are clever pedorthic lacing techniques that allow the tongue to expand around the bony prominence. Shoes with nonrigid toe box material and good toe height are also beneficial as cavus feet often develop hammertoes. Lateral wedges can be added to the midsole of some shoes to improve control. Lateral flares, providing a wider base of support, resist inversion and ankle torque. In more severe cases shoes may incorporate lifts for equinovarus type conditions and include long, high lateral counters. Finally, short articulating AFOs or leather ankle gauntlets can be prescribed to control recurring inversion sprains.
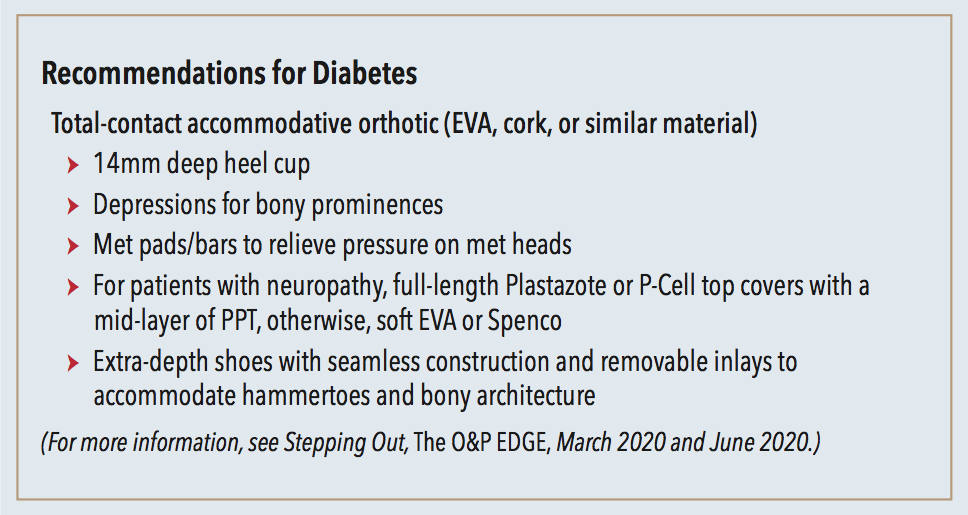
Diabetes
Ulcerations and other complications of the foot are some of the most serious and costly ramifications of diabetes mellitus. In response to the critical need for the prevention of foot ulcers, the International Diabetes Federation created an extensive archive of material and references for healthcare practitioners.3 Knowing peripheral neuropathy is the primary risk factor for the development of foot ulcers, their Diabetic Foot Screening Pocket Chart is an excellent guide to quickly evaluate and determine a patient’s risk category.
Part of the challenge in treating diabetes is that complications develop gradually. This frequently creates a false sense of complacency and patients feel no immediate reason to change diet or exercise habits. This is a dangerous assumption as neuropathy is irreversible. Initially the sense of vibration is lost. As sensation diminishes, the effects of motor neuropathy and position sense also begin to take hold. The biomechanics change when the small muscles of the foot become affected, creating weakness, atrophy, and imbalance. Further progression can limit joint mobility and the ability to walk, which sets off a cycle of less exercise leading to difficulty regulating weight and blood sugars.
Total-contact orthotics evenly distribute load and can be made with reliefs for areas of high pressure. The right choice of materials will provide cushioning, reduce shearing friction, and protect the skin from breakdown. They will also help control foot position and reduce excessive pronation. Accommodative foot orthotics are made from a variety of materials such as EVAs, crepes, and corks. Deep heel cups and sometimes flanges help cradle the foot and provide stability. Soft top covers protect the skin. Plastazote or P-Cell are often the first choice, but they do need to be refurbished frequently before completely wearing down.
People with diabetes must take special care with their footwear, especially if they are insensate. Good shoes must be well fitting with sufficient space in the front—both the length of the shoe and the height of the toe box. The toes should be covered to protect the digits and the shoe should have a sufficiently stabilizing heel counter. The inside should be seamless, particularly in the forefoot. Extra-depth shoes with removable inlays allow the practitioner to modify the existing insole redistributing pressure. Depth construction will also accommodate a custom orthotic if one is prescribed. Patients should be advised to change their shoes daily, not wearing the same pair on consecutive days. This allows shoes to air out, drying any perspiration that may have accumulated, creating a less attractive environment for bacteria and fungus.
Other diagnoses and treatments will be considered in Part II of this series.
Séamus Kennedy, BEng (Mech), CPed, is president and co-owner of Hersco Ortho Labs, New York. He can be contacted via e-mail at seamus@hersco.com or by visiting www.hersco.com.
References are available at opedge.com.