Seeing and treating patients every day, O&P clinicians observe the benefits and understand the value of the care they provide. However, anecdotal evidence and success stories, regardless of how obvious and intuitive they may be, are not the basis for scientific progress. High-quality research and studies that demonstrate the validity and efficacy of interventions are the most objective way to communicate the wonderful and amazing work we do to enhance patients’ lives. This is the fourth article in a series that highlights papers regarding the effectiveness of foot orthotics (July 2011, September 2016, and March 2021). The summary of each paper was adapted directly from its abstract.
Pediatrics
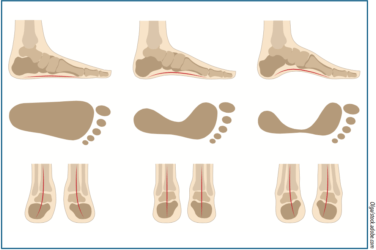
There are conflicting opinions within the medical community about when it is appropriate to treat pediatric flatfoot. This has been an ongoing conversation that swings between the poles of conservative early intervention or taking a wait-and- see approach. Both Wolff ’s Law (bone growth in response to force) and Davis’ Law (soft tissue modelling to imposed demands) support the assumption that misdirected repetitive stresses acting on vulnerable, young feet could lead to pathology. For example, a low-arched foot may be properly aligned and not exhibit any signs of pronation, but developmental flat feet appear normal when non-weight bearing yet collapse once the child stands. Although a child may be able to tolerate such an everted position—presenting as asymptomatic—there may be significant long-term consequences. Research suggests the beneficial use of foot orthotics as children’s feet go through a golden age where conservative treatment encourages normal development, setting them up for a lifetime of good exercise habits and pain-free walking.

1. Correction of hypermobile flatfoot in children by molded insert. 1980. Bordelon, R. L. The Journal of Foot and Ankle Surgery 1(3):143-50.
One hundred feet in 50 children between the ages of 3 and 9 years with a diagnosis of idiopathic hypermobile flatfoot had a custom-molded insert ordered. The insert was fabricated so that the standing lateral talometatarsal angle was corrected to neutral with the insert on the foot and the foot in the shoe. The preliminary reports indicate that a correction can be obtained at the rate of 0.41 degrees per month or approximately 5 degrees per year.
2. Relationship between “growing pains” and foot posture in children: single-case experimental designs in clinical practice. 2003. Evans, A. M. Journal of the American Podiatric Medical Association 93(2):111-7.
Eight complete single-case experimental designs were performed in the clinical setting. The in-shoe intervention proved efficacious for children with a pronated foot posture and aching legs. These findings may provide the impetus for a more rigorous examination of the possible relationship between pronation and “growing pains.”
3. Efficacy of custom foot orthotics in improving pain and functional status in children with juvenile idiopathic arthritis: a randomized trial. 2005. Powell M., Seid M., Szer I. S. The Journal of Rheumatology 32(5):943-50.
This study compared the clinical efficacy of custom foot orthotics, prefabricated off-the-shelf shoe inserts, and supportive athletic shoes worn alone on reducing pain and improving function for 40 children with juvenile idiopathic arthritis (JIA). In the conclusion, the authors state: In children with JIA, custom-made semi-rigid foot orthotics with shock-absorbing posts significantly improve pain, speed of ambulation, and self-rated activity and functional ability levels compared with prefabricated off-the-shelf shoe inserts or supportive athletic shoes worn alone.
4. Effect of foot orthoses on children with lower extremity growing pains. 2015. Lee, H. J., Lim, K. B., Yoo, J., Yoon, S. W., Jeong, T. H. Annals of Rehabilitation Medicine 39(2):285-93.
Twenty children with growing pains were recruited during a clinic visit. Resting calcaneal stance position (RCSP) and calcaneal pitch angle were measured, and individual custom-molded rigid foot orthoses were prescribed using the inverted orthotic technique to control for foot overpronation using the RCSP angle. Significant improvements were noted after one and three months in pain degree and frequency, and after three months in balancing ability. The paper concluded that the use of custom-molded foot orthoses is a good method for treating children with multiple musculoskeletal pains in the leg.
Diabetic Footcare
The brunt of the epidemic of diabetes can be measured financially and in terms of patient quality of life. With approximately 35 million people with diabetes in the United States and close to 90 million Americans with pre-diabetes, it will have profound effects on the nation’s healthcare system for decades. However, there is good evidence that the work orthotists, pedorthists, and podiatrists engage in every day are quite beneficial. Providing well-fitting extra depth shoes, Plastazote-covered total contact orthotics, and other interventions to relieve plantar pressure protect the at-risk foot. In addition, patient education and scheduled routine follow-ups are known to improve compliance and limit the most destructive aspects of the disease.


1. Effectiveness of diabetic insoles to reduce foot pressures. 1997. Ashry, H. R., Lavery, L. A., Murdoch, D. P., Frolich, M., Lavery, D. C. The Journal of Foot and Ankle Surgery 36(4):268-71; discussion 328-9.
Peak plantar pressures were measured in 11 people with diabetes each with a unilateral great toe amputation and an intact contralateral extremity (nonamputated), to evaluate the effectiveness of five footwear-insole strategies. Peak pressures under the first metatarsal, the lesser metatarsals, and the heel in feet with and without an amputation, as well as under the great toe on the contralateral foot were significantly reduced with insoles. There was no significant difference between the different insole modifications.
2. Effects of preventative footwear on foot pressure as determined by pedobarography in diabetic patients: a prospective study. 2001. R. Lobmann, R. Kayser, G. Kasten, U. Kasten, K. Kluge, W. Neumann, H. Lehnert Diabetic Medicine Apr;18(4):314-9.
This study analyzed the effects of specially manufactured insoles on foot pressures in patients with diabetes during a one-year prospective observation period. They studied 81 patients with type 2 diabetes without foot lesions. Eighteen patients with high-risk pressure received optimal insole support. Sixty- three patients as a control group received conventional footwear. After insole support a 30 percent pressure reduction of total foot Maximum Peak Pressure was achieved in the treatment group. After six months and one year, pressure reductions were still noted, although less than at the time of initial dispensing. The authors concluded that early insole support is successful in reducing plantar pressure. Repeated adjustments should be performed every six months to prevent foot pressure increases. In the control group a marked increase of the pressure values was found over the 12 months. Identification and subsequent support of patients with high ulceration risk may help to reduce the high amputation rate.
3. High plantar pressure and callus in diabetic adolescents. Incidence and treatment. Duffin, A. C., Kidd, R., Chan, A., Donaghue, K. C. 2003. Journal of the American Podiatric Medical Association 93(3):214-20.
Although subjects with diabetes were no more likely than control subjects to have high peak plantar pressure and callus, these anomalies place individuals with diabetes at greater risk of future foot problems. The effects of orthoses, cushioning, and both in combination were monitored in 17 subjects with diabetes with high peak plantar pressure and in 17 subjects with diabetes with plantar callus; reductions of up to 63 percent were achieved. Twelve-month follow-up of study subjects fitted with orthoses showed a significant reduction in peak plantar pressure even when the orthoses were removed. The subjects with diabetes who had not received any interventions dur- ing the same 12-month period showed no significant change in peak plantar pressure.
4. Effectiveness of insoles used for the prevention of ulceration in the neuropathic diabetic foot: a systematic review. 2011. Paton, J., Bruce, G., Jones, R., Stenhouse E. Journal of Diabetes and its Complications 25(1):52-62.
A total of five trials met the inclusion criteria: two randomized control trials (RCTs), two case control studies, and one follow-up study. Omitted details regarding the generalizability of results made study comparison and inference to practice difficult. There is a small amount of limited evidence indicating that insoles are effective in reducing incidence of ulceration and reducing plantar peak pressures in the diabetic neuropathic foot. In conclusion, insoles appear of use for the prevention of neuropathic diabetic foot ulceration, although evidence is limited. Clinical recommendation regarding type and specification of insole is not possible at this time. There is an essential need for a large well-designed RCT comparing different types of commonly used insole for the prevention of ulceration in the diabetic neuropathic foot.

Injury Prevention
Overuse injuries of the foot, ankle, and lower limb are quite common. Serious athletes, recreational exercisers, and certain trades and professions, among others, directly benefit from injury prevention. There are many risk factors for lower-limb injury, including biomechanics, overall patient health, and task-specific repetitive motions. Clearly any intervention that reduces downtime, prevents limitation of activities, or eliminates the cost of rehabilitation has direct value to the patient and the community.

1. Effects of short-term treatment strategies over 4 weeks in Achilles tendinopathy. 2007. Frank Mayer, Anja Hirschmüller, Steffen Müller, Martin Schuberth, Heiner Baur. British Journal of Sports Medicine 41(7):e6.
Thirty-one male runners with unilateral, untreated Achilles Tendinopathy (AT) completed four weeks of either physiotherapy, wearing custom fit semi-rigid insoles, or remained without treatment. Subjective pain as well as strength performance capacity was analyzed. The results showed pain was reduced to <50 percent of the baseline value after physiotherapy or after wearing insoles. Individual pain reduction was >50 percent in 89 percent of the insoles subjects, and 55 percent in those that received the physiotherapy. Conclusions: Most patients with AT experience a reduction in pain after only four weeks of differentiated, non-surgical treatment consisting of physiotherapy or semi-rigid insoles.
2. Foot orthoses in the prevention of injury in initial military training: a randomized controlled trial. Franklyn-Miller, A., Wilson, C., Bilzon, J., McCrory, P. 2011. The American Journal of Sports Medicine 39(1):30-7.
This was a randomized controlled trial designated as ‘Level of Evidence I.’ Four hundred military officer trainees were assessed by means of pressure plate, recording their contact foot pressures during walking. Participants were risk assessed and randomized to receive or not receive customized orthoses. Both cohorts were followed up for injury through their basic training at the seven-week point. The orthotic intervention group sustained 21 injuries in total (1 injury per 4,666 hours of training), whereas the control group sustained 61 injuries in total (1 injury per 1,600 hours of training) clearly demonstrating risk reduction with the use of orthoses. The conclusion was in this military trainee population, orthoses were effective in the prevention of overuse lower-limb injury.
3. A randomised control trial of short-term efficacy of in-shoe foot orthoses (prefabricated) compared with a wait-and-see policy for anterior knee pain and the role of foot mobility. 2012. Mills, K., Blanch, P., Dev, P., Martin, M., Vicenzino, B. British Journal of Sports Medicine 46(4):247-52.
This study investigated the short-term clinical efficacy of in-shoe foot orthoses over a wait-and-see policy in the treatment of anterior knee pain (AKP) and evaluated the ability of foot posture measures to predict outcome. There were 40 participants with clinically diagnosed AKP of greater than six-week duration, who had not been treated with orthoses in the previous five years. Prefabricated orthoses perceived as most comfortable from a selection of three different hardness values were provided compared with a wait-and-see control group. Foot orthoses produced a significant global improvement compared with the control group. Significant differences also occurred in measures of function. This study showed orthoses provide greater improvements in AKP than a wait-and-see approach.
4. Effectiveness of foot orthoses and shock-absorbing insoles for the prevention of injury: a systematic review and meta-analysis. 2017. Bonanno, D. R., Landorf, K. B., Munteanu, S. E., Murley, G. S., Menz, H. B. British Journal of Sports Medicine 51(2):86-96.
The authors conducted a systematic review and meta-analysis to investigate the evidence relating to the effectiveness of foot orthoses and shock-absorbing insoles for the prevention of musculoskeletal injury. Eleven trials that had evaluated foot orthoses and seven trials that had evaluated shock-absorbing insoles were included. Foot orthoses were found to be effective for preventing overall injuries and stress fractures but not soft-tissue injuries, while shock-absorbing insoles were not found to be effective for preventing any injury. However, further well-designed trials will assist the accuracy and precision of the estimates of risk reduction as the quality of the included trials varied greatly.
Many practitioners do not have the time to read research, but it is helpful to have articles and references close at hand. PubMed is a free resource supporting the search and retrieval of biomedical and life sciences literature. It is an excellent gateway to an immense body of work.
There are other ways to stay informed, up to date and connect with your peers. Consider joining one of the American Academy of Orthotists and Prosthetists’ (the Academy’s) Scientific Societies, being a reviewer for one of the professional journals, or offering your expertise to deliver educational lectures to other healthcare professionals. For the truly ambitious: Why not take that idea or observation you have been mulling over, do some research and get it published? Several organizations offer grants for funding research, including the American Board for Certification in Orthotics, Prosthetics & Pedorthics, the Orthotic and Prosthetic Education and Research Foundation, and the Pedorthic Foundation, or others listed in the Academy’s Research Funding Guide. Each step we take to improving the science of O&P, and sharing those results, strengthens the profession and the quality of life for our patients.
Séamus Kennedy, BEng (Mech), CPed, is president and co-owner of Hersco Ortho Labs, New York. He can be contacted via e-mail at seamus@hersco.com or by visiting www.hersco.com.